Relationship between serum IgA level and allergy/asthma
Article information
Abstract
Background/Aims
Mucosal immunoglobulin A (IgA) may prevent the entrance of allergens. This study examined the relationship between serum IgA levels (within the normal range) and sensitization to house dust mites (HDM) or airway hyper-responsiveness (AHR).
Methods
The clinical records of 1,136 adult patients with suspected asthma, for whom test data for serum IgA level and methacholine-AHR were available, were reviewed retrospectively. The AHR/allergy indices were compared among patient groups with low (<140 mg/dL, group I), intermediate (140 to 280 mg/dL, group II), or high (≥280 mg/dL, group III) IgA levels in serum.
Results
The HDM skin sensitization rate progressively decreased from 30.0% in group I (n = 139) to 26.8% and 18.5% in groups II (n = 684) and III (n = 313), respectively (p = 0.003). Although both the HDM sensitization degree and the IgA level were significantly related to age, the adjusted odds ratio (OR) of association of a high IgA level (≥ 280 mg/dL) with HDM sensitization was significant (0.617; 95% confidence interval [CI], 0.415 to 0.916; p = 0.017). Among younger subjects (≤ 45 years of age) with AHR, the prevalence of moderate/severe AHR progressively decreased (70.6%, 52.3%, and 47.1% in groups I, II, and III [n = 34, 149, and 51]), respectively (p = 0.045). The IgA < 140 mg/dL was a significant risk factor for moderate/severe AHR (OR, 2.306; 95% CI, 1.049 to 5.071; p = 0.038).
Conclusions
Sensitization to HDM and methacholine-AHR were significantly associated with serum IgA levels in suspected asthmatics, even when those levels were normal.
INTRODUCTION
Selective immunoglobulin A (IgA) deficiency, a common primary immunodeficiency, is not infrequently diagnosed in Caucasians (prevalence, 1:300 to 3,000) [1]. In subjects with IgA deficiency, not only is the incidence of recurrent infections very high but the incidence of atopic diseases was also reported to be high as early as 1980 [2]. Therefore, over many years, our team has routinely screened serum IgA levels to detect IgA deficienciences in patients with suspected allergic diseases, even though selective IgA deficiency may be very rare in Koreans; the prevalence thereof was only 1:14,840 in Japanese [3].
Later, Ludviksson et al. [4] reported that asthma was significantly more common and allergic symptoms more severe in infants with low IgA levels, although the levels were normal for age. In addition, infants born to atopic parents had a higher prevalence of salivary IgA deficiency [5]; children with positive skin prick tests to common allergens had lower serum IgA levels; and children who developed allergic rhinitis or atopic eczema had lower salivary IgA levels [6].
Mucosal IgA neutralizes bacteria and viruses by interfering with epithelial adhesion and improving the properties of mucus in trapping and removing antigens (immune exclusion) [7]. Therefore, recurrent (usually bacterial) infections are associated with IgA deficiency [2,8]. Via the same mechanism, IgA may also prevent the development of allergic inflammatory reactions to environmental allergens. In fact, pretreatment with short ragweed-specific IgA prevented the development of lung eosinophilia and airway hyper-responsiveness (AHR) after airway challenge with ragweed in mice [9]. Atopics may have insufficient amounts of IgA, and so may be prone to development of allergic diseases. During early life, when the human immune system is immature, impaired IgA responses may facilitate sensitization to allergens and the development of allergic diseases. Therefore, the subjects of many studies on IgA/ allergy were infants or children [2,4-6]. In adulthood, IgA levels may be restored to normal and reduced IgA levels in nasal washes of adult asthmatics were not evident in one study [7]. However, Balzar et al. [10] reported that serum IgA levels correlated with asthma severity in adult asthmatics.
Asthma is a disease characterized by AHR. The house dust mites (HDM) Dermatophagoides pteronyssinus (Dp) and Dermatophagoides farinae (Df) are well-known to be the most common allergens causing asthma, and the relative risk for AHR of sensitization to HDM is 4.45 [11]. Although Papadopoulou et al. [12] showed that AHR associated with HDM sensitization occurred frequently in children with selective IgA deficiency, no work has yet shown any relationship between serum IgA levels within the normal range and HDM sensitization/AHR. Therefore, the present study was designed to explore the relationships between serum IgA levels (including those within the normal range) and HDM sensitization or AHR in adult asthmatics.
METHODS
Subjects
The clinical records of 1,136 adult patients with suspected asthma, for whom serum IgA levels were available, and who underwent the methacholine-AHR test in the Division of Allergy of a tertiary hospital between 2007 and 2013, were retrospectively reviewed. Suspected asthma was defined as asthma-like symptoms suspected by a doctor. The intervals between both tests for all subjects were less than 4 months. No subject met the international definition of selective IgA deficiency (serum IgA < 7 mg/dL) [13], and only six of 1,136 subjects exhibited a subnormal IgA level (7 to 70 mg/dL) as defined by Weber-Mzell et al. [1]. All subjects were divided arbitrarily into three groups by reference to serum IgA level: low (< 140 mg/dL, twice the lower limit of normal, group I); intermediate (140 to 280 mg/dL, group II); or high (≥ 280 mg/dL, four times the lower limit of normal, group III).
Lung function tests
Lung function tests were performed using a computerized spirometer (Spiro Analyzer ST-250, Fukuda Sanyo, Tokyo, Japan) according to the method recommended by the Intermountain Thoracic Society [14]. Each predicted value of the forced expiratory volume in 1 second (FEV1) was calculated using the regression equation of Crapo et al. [15].
The test for AHR to methacholine (Sigma-Aldrich, St. Louis, MO, USA) aerosolized using a DeVilbiss 646 jet nebulizer (DeVilbiss Co., Somerset, PA, USA; output 0.13 mL/min) was performed using the standardized tidal breathing method [16]. The concentration of methacholine causing a 20% fall in FEV1 (PC20, mg/mL) was obtained via linear interpolation from a log dose-response curve. The severity of methacholine-AHR was scored using a modification of the method of Woolcock and Jenkins [17], as follows: PC20 > 16 (normal, score 0); 2 to 16 (mild, 1); 0.2 to 2 (moderate, 2); and < 0.2 mg/mL (severe, 3).
Blood tests
IgA and immunoglobulin E (IgE) serum levels (normal: 70 to 400 mg/dL and < 100 IU/mL, respectively) were measured by nephelometry (Behring Diagnostics GmbH, Marburg, Germany). White blood cell counts and the percentages and numbers of eosinophils (white blood cell count × eosinophil %) in peripheral blood were also measured. An elevated eosinophil count (eosinophilia) was defined as ≥ 450 cells/μL [18].
Allergy skin prick tests
Allergy skin prick tests were performed using 55 common allergens, including HDM Dp and Df. A histamine solution (1 mg/mL) served as a positive control and normal saline as a negative control. Wheal and flare sizes were measured 15 minutes after the application of test agents. Mean values were calculated from the largest and smallest diameters of wheals measured at right angles to each other. The skin sensitivity grade to a specific allergen was determined by calculating the ratio of the size of the wheal induced by the allergen to the size of that induced by the histamine solution, as follows: 25% to 50%, 1+; 50% to 99%, 2+; 100% to 199%, 3+; and ≥ 200%, 4+. In subjects who did not exhibit dermographism, a sensitivity grade ≥ 3+ was considered to be clinically significant.
Statistical analysis
Data from groups divided by serum IgA levels were analyzed by one-way analysis of variance and are presented as means ± standard errors. Multiple comparisons using the Tukey method were made during post hoc testing. Proportions were compared among groups using the chi-square test for trend (the linear-by-linear association). Correlations among variables were assessed by calculating Pearson correlation coefficients. The relative risks of HDM sensitization and moderate/severe AHR were assessed via logistic regression. Statistical analyses were performed using SPSS for version 20.0 (IBM Co., Armonk, NY, USA), and a p value of < 0.05 was considered to indicate statistical significance.
RESULTS
Relationship between serum IgA levels and other variables
Among the 1,136 subjects, the serum IgA levels were low (< 140 mg/dL, group I) in 139 patients (12.2%); intermediate (140 to 280 mg/dL, group II) in 684 (60.2%); and high (≥ 280 mg/dL, group III) in 313 (27.6%) (Table 1). The mean serum IgA levels were 114, 208, and 354 mg/dL in the three groups, respectively. There was no significant difference among groups in terms of the proportions of males and eosinophilia, and the baseline FEV1. However, the age of the group III was significantly higher than those of groups I and II. Higher IgA levels were associated with greater proportions of subjects with increased serum total IgE levels, and (inversely) with lower proportions of subjects sensitized to HDM Dp or Df (30.0%, 26.8%, and 18.5%, respectively; X2 = 8.550, p = 0.003). The proportion of subjects sensitized to Dp progressively fell in those with higher IgA levels, as was also true of subjects sensitized to Df (both p < 0.01) (Fig. 1). The numbers of allergens yielding positive reactions in skin tests tended to decrease as the serum IgA level increased although statistical significance was not attained (p = 0.097). We found no significant difference in the distributions of subjects with moderate/severe AHR among groups classified by serum IgA level.

Clinical characteristics of suspected asthma patients classified according to the serum IgA level

Proportion of subjects sensitized to house dust mites (A) Dermatophagoides pteronyssinus (Dp) and (B) Dermatophagoides farinae (Df) in adult suspected asthma patients grouped according to their serum immunoglobulin A (IgA) levels.
The serum IgA level correlated positively with age (r = 0.140, p = 0.000) (Table 2). A higher IgA level was associated with lower numbers of sensitized allergens (r = –0.061, p = 0.049) and lower-grade sensitivity to HDM Dp/Df (r = –0.093, p = 0.003). Unexpectedly, we found a positive correlation between the serum level of IgA and total IgE (r = 0.110, p = 0.000). None of the blood eosinophil %, FEV1, or AHR was significantly associated with the serum IgA level.
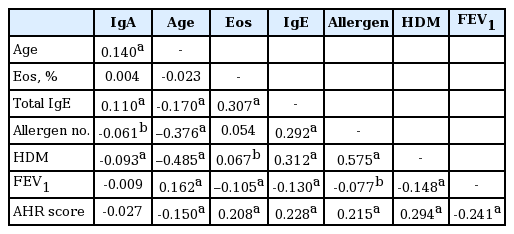
Correlation coefficients among variables in suspected asthma patients
Age was significantly associated with total IgE level, the number of allergens, HDM sensitivity grade, FEV1, and AHR severity. There were significant relationships among the allergy markers, FEV1, and AHR.
Relative risk of sensitization to house dust mites
Increased serum IgA levels significantly reduced the relative risk of sensitization to HDM Dp or Df (odds ratio [OR], 0.998; p = 0.012) (Table 3). A low IgA level (< 140 mg/dL) was not significantly associated with an increased risk of HDM sensitization, but a high IgA level (≥ 280 mg/dL) was significantly associated with a decreased risk thereof (OR, 0.599; p = 0.003). In addition, greater age and better lung function were associated with lower risk, but all of male sex, increased serum total IgE level, and moderate/severe AHR were risk factors for HDM sensitization. However, the age of male subjects (n = 492) was significantly less than that of female subjects (n = 644; 42.6 ± 0.8 years vs. 53.2 ± 0.6 years, p = 0.000), and the IgA level did not significantly differ between the sexes (237 ± 4 mg/dL vs. 237 ± 4 mg/dL, p = 0.936). Upon multivariate regression analysis, the risks for HDM sensitization of an IgA level ≥ 280 mg/dL (OR, 0.617; p = 0.017), greater age, and increased serum total IgE level were statistically significant.
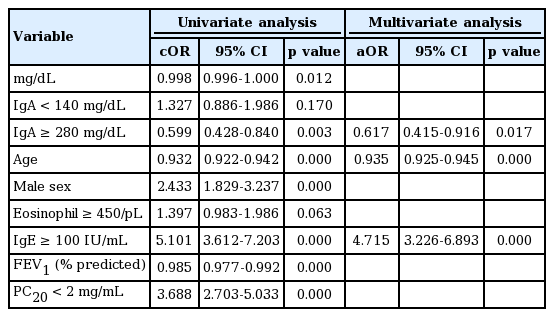
Relative risk for skin sensitization to house dust mites Dermatophagoides pteronyssinus or Dermatophagoides farina in suspected asthma patients
The relationship between serum IgA level and AHR in young subjects with AHR
As we found no significant relationship between IgA level and AHR, and as both the IgA level and AHR were associated with age, the subjects aged ≤ 45 years were selected for analysis of AHR data to exclude any effect of age. Some such subjects (such as those with allergic rhinitis) might have become sensitized to HDM without development of AHR and, thus, young asthma patients with AHR (n = 234) were selected to assess the risk of moderate/severe AHR. No significant difference in age among groups classified in terms of serum IgA level was noted: the age was 26.7 ± 1.5 years in the low IgA group (< 140 mg/dL, n = 34); 29.4 ± 0.8 years in the intermediate IgA group (140 to 280 mg/dL, n = 149); and 30.5 ± 1.1 years in the high IgA group (≥ 280 mg/dL, n = 51). However, higher serum IgA levels were associated with lower proportions of subjects with moderate/severe AHR: 24/34 (70.6%), 78/149 (52.3%), and 24/51 (47.1%) in the three groups, respectively (X2 = 4.008, p = 0.045) (Fig. 2).

Proportion of subjects with moderate/severe airway hyper-responsiveness (AHR; i.e., the provocative concentration of methacholine causing a fall in forced expiratory volume in 1 second < 2 mg/mL) in young (≤ 45 years-old) adult asthma patients with AHR (n = 234) grouped according to their serum immunoglobulin A (IgA) levels.
A low IgA level was a significant risk factor for moderate/severe AHR (OR, 2.306; p = 0.038) (Table 4). In addition, although greater age and better lung function were associated with lower risk, all of male sex, eosinophilia, increased serum total IgE level, and HDM sensitization, were all significant risk factors for moderate/severe AHR. However, the mean age of males (n = 155) in our study was significantly lower than that of females (n = 79) (27.0 ± 0.7 years vs. 33.6 ± 1.0 years, p = 0.000), and the IgA level did not significantly differ between the sexes (219 ± 7 mg/dL vs. 225 ± 11 mg/dL, p = 0.660). Upon multivariate regression analysis, HDM sensitization and lung function were significantly associated with AHR.

Relative risk for moderate/severe airway hyper-responsiveness (methacholine PC20 < 2 mg/mL) in young (≤ 45 yearsold) asthma patients (n = 234)
DISCUSSION
In the present study, the serum IgA levels in almost all subjects were within the normal range; however, the rate and extent of HDM sensitization were significantly (inversely) related to the serum IgA level. Similarly, the prevalence of moderate/severe AHR was also significantly (inversely) related to the IgA level in asthmatics. These results are consistent with those of previous studies [2,4-6,10] showing that low IgA level is associated with atopic disease. The subjects of previous studies [2,4-6] were mainly children, and some authors have found that the atopy/IgA relationship was unclear in adult patients [7]. However, a study in adult patients by Balzar et al. [10] revealed a relationship between serum IgA level and asthma severity. Similarly, we found a relationship between serum IgA level and allergy/asthma. To our knowledge, this is the first study worldwide to show that serum IgA levels within the normal range are associated with sensitization to HDM and AHR.
Mucosal IgA may be insufficient to prevent the entrance of allergens via the mucosa, resulting in the ready development of allergic diseases in atopic subjects [5,6]. Recently, it has been reported that IgA may play an important role in the context of the so-called “hygiene hypothesis,” suggested to be the principal mechanism explaining the recent abrupt worldwise increase in the prevalence of allergic diseases including asthma. When Fageras et al. [19] examined children born in Sweden and Estonia at 3, 6, and 12 months, and at 2 and 5 years of age, the children in Sweden, where respiratory infections were less prevalent than in Estonia, showed a higher prevalence of allergic disease (47% vs. 24%), and positive skin prick test results (41% vs. 21%), and lower secretory IgA levels in saliva, than did children in Estonia. Low microbial pressure might cause the IgA system to mature more slowly in Swedish children. In addition, it has been shown that the beneficial effects of grass pollen-specific subcutaneous [20] or sublingual [21] immunotherapy were associated with induction of specific IgA2. In a murine asthma model, HDM Df-specific sublingual vaccine pre-treatment protected from development of AHR and eosinophilic airway inflammation in association with increased response of Df-specific IgA [22].
Although all subjects in the present study underwent AHR testing because of suspected asthma manifestations, only 500 of the 1,136 patients (44.0%) exhibited AHR. Therefore, in all subjects, HDM sensitization, but not AHR, was associated with the serum IgA level. Both asthmatics and allergic rhinitis patients without AHR may become sensitized to allergens under the influence of serum IgA level, and thus, the relationship between the HDM sensitization and the IgA level may become significant. However, the influence of serum IgA level on AHR may be obscured by enrollment of allergic rhinitis patients without AHR. In addition, age was significantly related to both serum IgA level and AHR. Moreover, unlike “variable” AHR mediated by inflammation, “persistent” AHR caused by remodeling is not affected readily by any factor including serum IgA level [23], and “persistent” AHR would be more predominant at older ages. Therefore, when we selected young asthmatics with AHR to avoid the effects of such confounding factors, we found that the prevalence of moderate/severe AHR was significantly related to the serum IgA level.
None of our subjects had selective IgA deficiency, and only six (0.5%; compared to 2.13% in healthy Caucasians [1]) exhibited subnormal IgA levels or partial deficiencies. We may have underestimated the prevalence of deficiency. When the relationship between AHR and IgA level is considered, some subjects with severe asthma who could not undergo AHR testing may possibly have had IgA deficiencies. If severe asthmatics had been included as study subjects, the relationship between serum IgA levels and AHR/asthma would have been more apparent. Thus, Balzar et al. [10] demonstrated a significant relationship between serum IgA level and forced vital capacity (rs = 0.65, p = 0.002). In addition, in line with the concept of “variable AHR,” eosinophilia was a significant risk factor for moderate/severe AHR in the present study. Choi et al. [24] showed that Bacille Calmette-Guérin vaccination was effective to treat active, but not silent, asthma (eosinophilia is a marker of activity). Thus, any relationship between IgA level and AHR would be more apparent in subjects with active asthma.
The serum IgA level was positively associated with age. Fageras et al. [19] reported that salivary IgA levels in children increased with age, attaining adult levels by the age of 5 years. In adults also, serum IgA levels increase with age by an average of 2 mg/dL per year [1]. As postnatal microbial pressure may induce salivary IgA production in children [19], repeated infections in adulthood also may induce a progressive increase in serum IgA levels with age. If so, the well-known fact that the odds of yielding a positive skin test to common aeroallergens decreases (on average) by 2.11% per year [25] may be at least in part explained by the increase in serum IgA level with age in consequence of repeated microbial exposures.
Male sex was a risk factor for HDM sensitization and moderate/severe AHR in the present study. However, our male subjects were younger than the female subjects, and we found no sexual difference in serum IgA level. The main reason why the data indicate (probably falsely) that male sex is a risk factor would be that age profoundly affected our results, because younger subjects more frequently exhibit allergic sensitization [25] and, in turn, AHR. Although boys seem to be more easily sensitized to HDM in childhood than do girls [26], females of child-bearing age (mostly adults) are more likely to be sensitized to HDM and to suffer from allergic asthma [27]. Weber-Mzell et al. [1] reported that serum IgA levels were higher in males than in females. As the IgA level increases with age, and as our male subjects were younger than our female subjects, any sexual difference in IgA level may have been obscured in the present study. In general, such a subject-selection bias may be a weak point of any cross-sectional study, as in our present work.
Even though the serum total IgE level was positively associated with the degree of HDM skin sensitivity, and inversely with age (skin sensitivity decreases generally with age [25]), that level (surprisingly, in contrast to the HDM sensitivity) was positively related to the serum IgA level. In the work of Ludviksson et al. [6], both IgA and IgE levels in serum increased from 2 to 4 years of age, probably because of progressive maturation of plasma cells, and these levels were positively associated even though serum IgA levels were significantly lower in skin test-positive children 2 years of age. Likewise, we noted that some patients with high IgE levels tended to have high IgA levels, and those with low IgE levels low IgA levels, suggesting individual differences in plasma cell functioning, caused either by aging or other factors. In addition, unlike HDM sensitization, serum total IgE levels may be increased by parasitic infestations and may be associated, in adults, with the development of other diseases such as allergic bronchopulmonary aspergillosis and Churg-Strauss syndrome.
Secretory IgA in mucosa is mainly composed of IgA2, but in serum, IgA1 is dominant [7]. Patients with optimal levels of serum IgA always have secretory IgA antibodies in their secretions [28]. Fageras et al. [19] showed that secretory IgA was the principal form of IgA in the saliva of Estonian children, but was present at insufficient levels in Swedish saliva. Therefore, further studies on secretory IgA rather than serum IgA are required.
In summary, sensitization to HDM in patients with suspected asthma was significantly related to the serum IgA level, even when that level was normal. In addition, the prevalence of moderate/severe AHR progressively decreased with an increase in serum IgA level in young asthmatics with AHR. IgA may prevent sensitization to HDM and development of AHR in asthmatic patients.
KEY MESSAGE
1. The prevalences of sensitization to house dust mites and airway hyper-responsiveness were related to the serum immunoglobulin A level even that level was within the normal range.
Notes
No potential conflict of interest relevant to this article was reported.