Quantitative analysis of nailfold capillary morphology in patients with fibromyalgia
Article information
Abstract
Background/Aims
Nailfold capillaroscopy (NFC) has been used to examine morphological and functional microcirculation changes in connective tissue diseases. It has been demonstrated that NFC patterns reflect abnormal microvascular dynamics, which may play a role in fibromyalgia (FM) syndrome. The aim of this study was to determine NFC patterns in FM, and their association with clinical features of FM.
Methods
A total of 67 patients with FM, and 30 age- and sex-matched healthy controls, were included. Nailfold capillary patterns were quantitatively analyzed using computerized NFC. The parameters of interest were as follows: number of capillaries within the central 3 mm, deletion score, apical limb width, capillary width, and capillary dimension. Capillary dimension was determined by calculating the number of capillaries using the Adobe Photoshop version 7.0.
Results
FM patients had a lower number of capillaries and higher deletion scores on NFC compared to healthy controls (17.3 ± 1.7 vs. 21.8 ± 2.9, p < 0.05; 2.2 ± 0.9 vs. 0.7 ± 0.6, p < 0.05, respectively). Both apical limb width (µm) and capillary width (µm) were significantly decreased in FM patients (1.1 ± 0.2 vs. 3.7 ± 0.6; 5.4 ± 0.5 vs. 7.5 ± 1.4, respectively), indicating that FM patients have abnormally decreased digital capillary diameter and density. Interestingly, there was no difference in capillary dimension between the two groups, suggesting that the length or tortuosity of capillaries in FM patients is increased to compensate for diminished microcirculation.
Conclusions
FM patients had altered capillary density and diameter in the digits. Diminished microcirculation on NFC may alter capillary density and increase tortuosity.
INTRODUCTION
Fibromyalgia (FM) syndrome, characterized by chronic diffuse muscle pain, skin sensitivity, sleep disturbance, depression, anxiety, and fatigue [1], is also accompanied by a variety of other symptoms, including migraines, interstitial cystitis, irritable bowel syndrome and vasospastic symptoms [2]. Vasospastic symptoms in FM include Raynaud's phenomenon and intolerance to cold, caused by decreased microcirculatory blood flow above tender points [3]. Therefore, slight morphological changes in nailfold capillaries may occur in FM patients [4].
Nailfold capillaroscopy (NFC), a modality used to diagnose secondary Raynaud's phenomenon, can be used to examine morphological and functional microcirculation changes in connective tissue diseases (CTDs) [5]. Raynaud's phenomenon develops during early-stage CTD; it is observed in 80% to 90% of systemic sclerosis (SSc) patients such that early diagnosis is very important. Examination of the nailfold capillaries can reveal the nature and extent of microvascular pathology in patients with CTD. Several prominent nailfold capillary changes, including mega-capillary, capillary hemorrhage, and loss of capillary distribution, are clearly apparent in SSc [6].
Several studies have examined NFC patterns in FM patients, including a report from Morf et al. [4]. However, compared to SSc, there has been insufficient research concerning findings on NFC, although many FM patients suffer from Raynaud's-like symptoms. Therefore, this study compared NFC findings between FM patients and healthy controls, and investigated NFC patterns in FM and the association between these patterns and the clinical features of FM.
METHODS
Patient selection
A total of 67 patients were randomly selected from those fulfilling the 1990 American College of Rheumatology (ACR) criteria for FM, who first visited our outpatient clinic; 30 age- and sex-matched healthy controls were also included in this study.
Investigations of clinical manifestations
Clinical parameters included tender point count, Fibromyalgia Impact Questionnaire (FIQ) score [7], arthralgia, headache, sensations of numbness or coldness, irritable bowel syndrome, dry eyes, and dry mouth. The FIQ comprises 10 brief, self-administered scales as follows: physical impairment, feeling good, missing work, completing work, pain, fatigue, feeling rested, stiffness, anxiety, and depression.
Nailfold capillaroscopy
Before the nailfold test, patients were seated inside the procedure room for a minimum of 15 minutes to adapt to the room temperature of 20℃ to 25℃. Each patient was seated such that the dorsum of their hand was facing upwards, with halogen lights illuminating the nails (coated with immersion oil) under nailfold microscopy. The NFC test was performed by a skilled examiner who was not aware of the patients' clinical status. Patients' nailfolds, of the second, third and fourth digits of both hands, were observed under a light microscope (×100 and ×400 magnifications; Olympus SZ-PT, Olympus, Tokyo, Japan). A digital camera (Polaroid, Minnetonka, MN, USA) transmitted all microphotographs to a computer; after the images were saved, they were enhanced using color filtering via the Adobe Photoshop version 7.0 (Adobe Systems Inc., San Jose, CA, USA). For quantitative analysis, we counted the total number of capillaries, and the number of deletions, within a 3-mm-wide area of the central part of the digits [8]. The outcomes were recorded as average values for six digits. Furthermore, an experienced rheumatologist measured the apical limb width, and the capillary width, of three capillary rings located at the center (where the resolution is most-fine), directly from a computer screen and from all six digits. By measuring the capillary boundary at a capillary length of 25 µm (1 cm; ×400) we defined the capillary dimension as the total number of pixels in the designated area (Fig. 1) [6], using the Adobe Photoshop version 7.0.
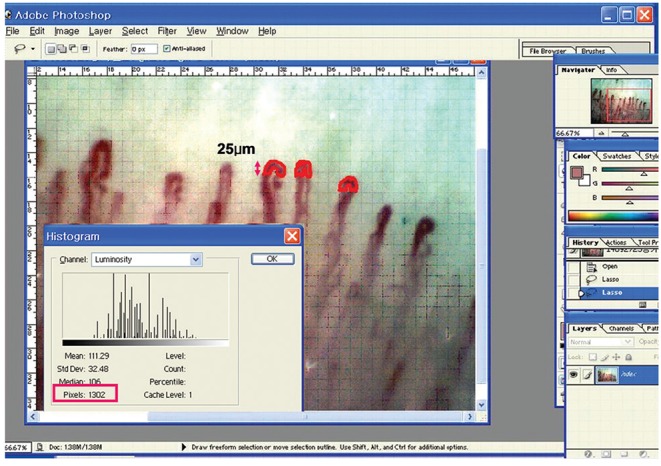
Method for calculating "total pixel number" using the Adobe Photoshop version 7.0 (Adobe Systems) as a function of capillary dimension. A perpendicular length of 25 µm tangential to the internal limit of a capillary loop transverse segment was defined as the transverse segment area. Adapted from Kim et al. [6] with permission from Springer.
Statistical analysis
All results are expressed as median values and interquartile ranges. For statistical analysis, the SPSS version 13.0 (SPSS Inc., Chicago, IL, USA) was used. We used the Mann-Whitney U test to compare NFC parameters and FIQ scores; Fisher exact test and the chi-square test were used to compare clinical manifestations between the FM patient and control groups. Spearman correlation coefficient was used to assess the relationship between NFC measurement parameters and FIQ scores. A p < 0.05 was taken to indicate statistical significance.
RESULTS
Demographic and clinical characteristics of fibromyalgia patients
We included a total of 67 FM patients and 30 healthy controls. The mean age of the 67 FM patients was 41.97 years, compared to 37.26 years in the 30 healthy controls. There were 63 females (94%) in the FM group; all 30 healthy controls were female. Mean body mass index was marginally higher in the FM group (22.46 kg/m2) compared to the control group (21.9 kg/m2). A total of six FM patients (8.96%) had Raynaud's phenomenon, which represents a significantly higher prevalence rate compared to that of the control participants (none of whom had Raynaud's phenomenon). The mean duration of Raynaud's phenomenon in the FM group was 8.1 months (Table 1).

Demographic characteristics and features of Raynaud's phenomenon in the control and fibromyalgia syndrome groups
The most frequent symptom observed in the FM group was arthralgia (n = 47, 70.1%) followed by headache (n = 39, 58.2%), numbness (n = 38, 56.7%) and peripheral coldness (n = 34, 50.7%). Other symptoms or syndromes in the FM patients included irritable bowel syndrome (n = 31, 48.3%), dry eye (n = 20, 29.9%), and dry mouth (n = 15, 22.4%). More than 50% of the FM group were full-time housewives; 41 of this group (61.2%) were working from home, whereas 26 (38.8%) had other occupations. Six (9.0%) of these FM patients were employees, three (4.5%) were laborers, five (7.5%) were operators, and 12 (70.1%) had other jobs. A total of 47 (70.1%) FM patients were married and 24 (35.8%) were postmenopausal (Table 2).
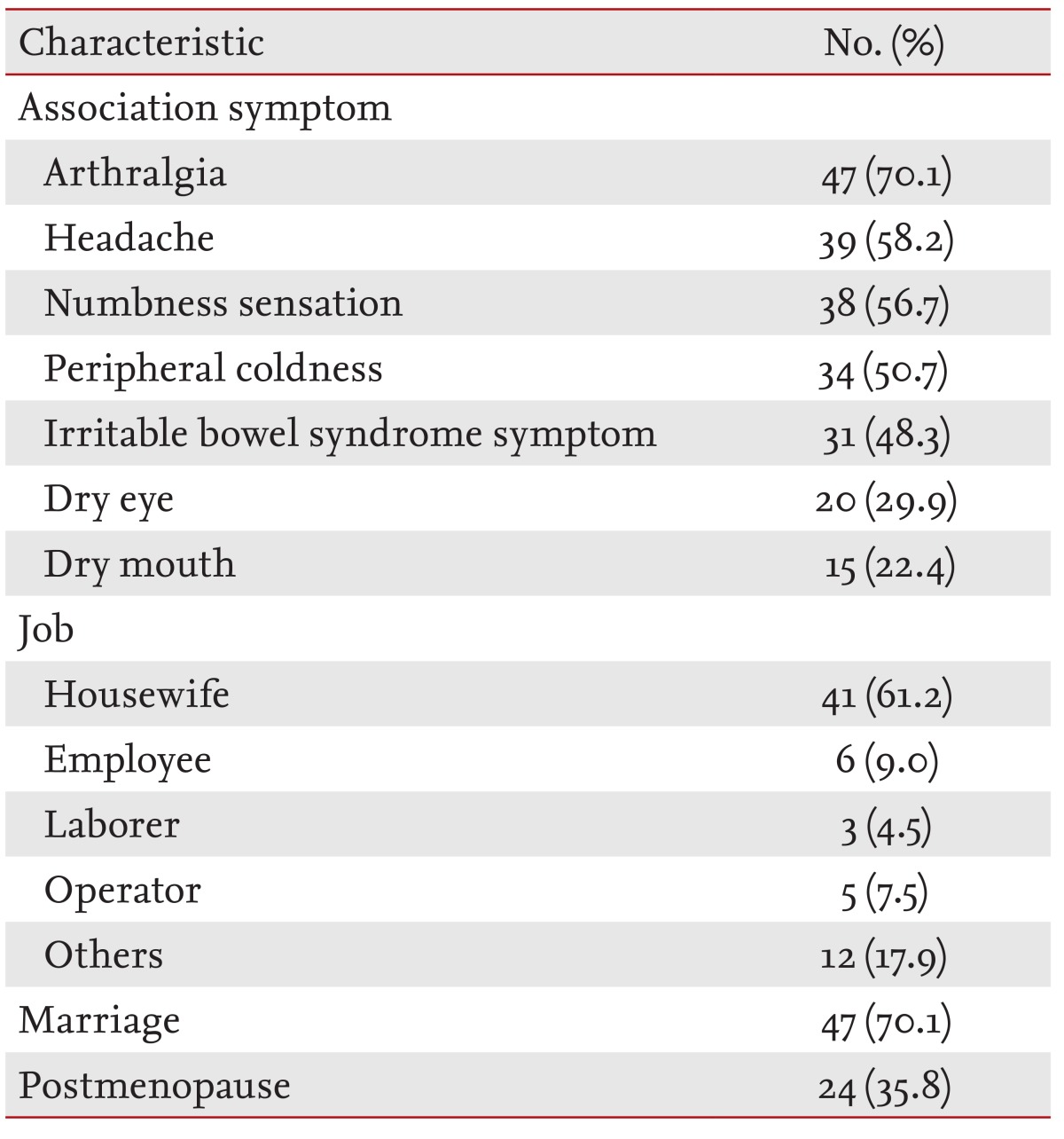
Clinical and demographic characteristics of the fibromyalgia syndrome group (n = 67)
FIQ scores in fibromyalgia participants
FIQ was designed to assess the current health status of FM patients across diverse domains, including physical function and symptoms. The FIQ consists of 10 subscales, the first of which comprises 11 items related to the performance of physical functions that require significant muscular exertion. The second and the third subscales are concerned with the number of days on which patients felt well, and the number of days on which they were unable to work (including housework) due to FM symptoms. Subscales 4 to 10 represent horizontal linear scales assessing work difficulty, pain, fatigue, morning tiredness, stiffness, anxiety, and depression [9]. Our FM groups completed the FIQ subscales concerned with their physical functionality and symptoms (Table 3).
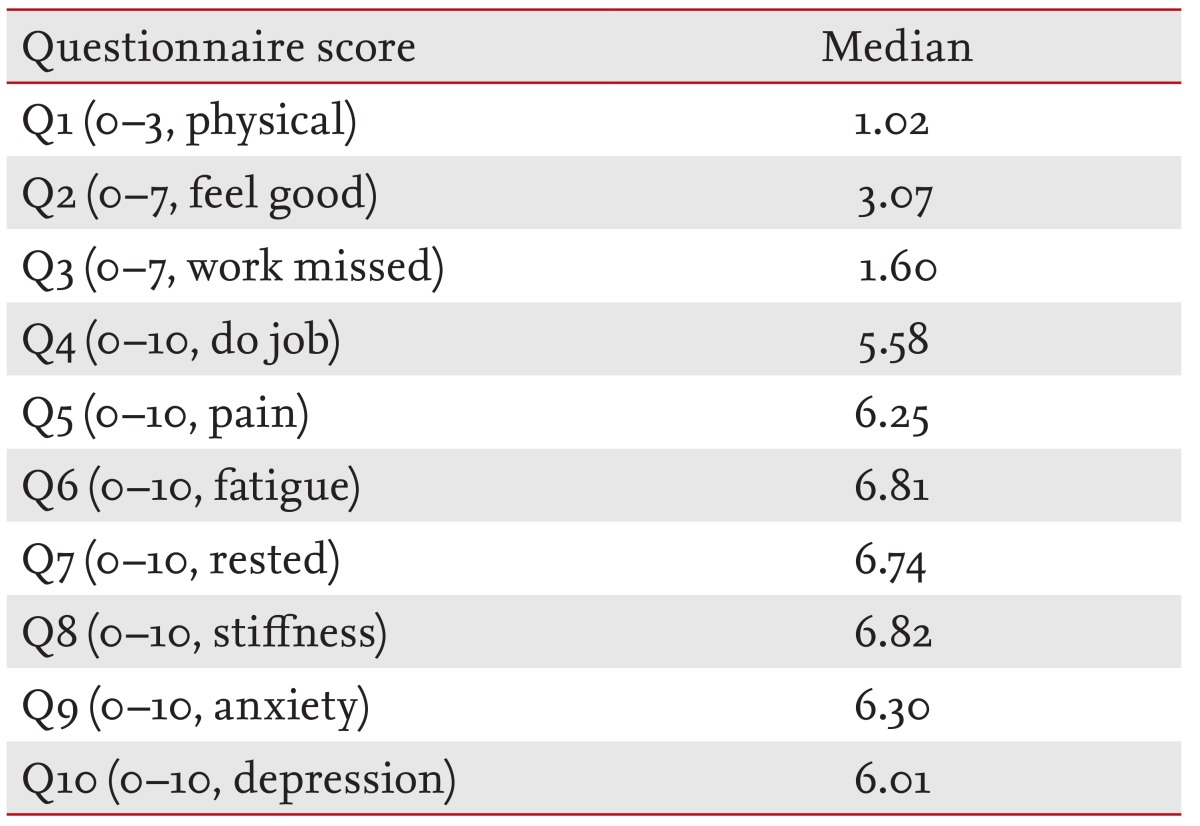
Fibromyalgia Impact Questionnaire scores in the fibromyalgia syndrome group (n = 67)
Nailfold capillary microscopic features in the FM and healthy control groups
We conducted the NFC test on both the FM and healthy control groups. The FM patients had an average of 17.3 ± 1.7 loops in the 3-mm-wide area of the central part of their digits, compared to an average of 21.8 ± 2.9 loops in the control group. The average number of loop deletions was 2.2 was 2.2 ± 0.9 in the FM group, compared to 0.6 ± 0.7 in the healthy controls (Table 4). It appears that FM patients had a lower number of capillaries, but higher deletion scores compared to the healthy controls on NFC. The average apical width (µm) of the FM patients was 1.1 ± 0.2; their mean capillary width (µm) was 5.4 ± 0.5. In the control group, the average apical width was 3.7 ± 0.6; their capillary width was 7.7 ± 1.4 (Table 4). Both apical limb and capillary width were significantly decreased in FM patients, indicating that FM patients have abnormally decreased digital capillary diameter and density.
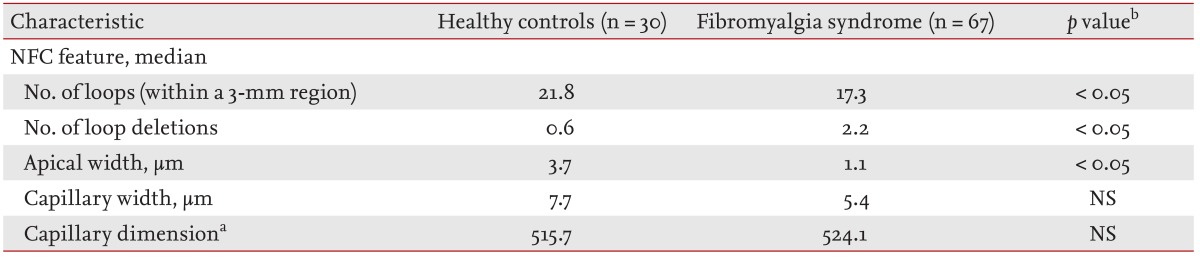
Microscopic nailfold capillary characteristics
However, capillary dimension (total number of pixels measured using Adobe Photoshop) did not differ between the FM and control groups. The mean capillary dimension of the FM group was 524.1 pixels; in the control group it was 515.7 pixels (Table 4). This suggests that the length or tortuosity of capillaries in FM patients is increased to compensate for diminished microcirculation.
Correlation between clinical manifestation and nailfold capillary microscopic parameters
To compare the FIQ scores of each group with their NFC results, we assessed the correlations between clinical manifestations and NFC parameters; as shown in Table 5, among the FIQ parameters, only subscale 1 (physical function) was negatively correlated with capillary dimension (r = -0.248, p = 0.048); there were no other significant associations between NFC patterns and other FIQ subscale scores.

Correlation of clinical manifestations with nailfold capillary microscopic parameters
DISCUSSION
FM is a chronic pain syndrome defined by widespread pain for > 3 months and the presence of ≥ 11 of 18 tender points [10]. In 2010, the ACR announced revised FM diagnostic criteria, designed for primary and specialty care, to diagnose FM simply and practically and to provide a severity scale for characteristic FM symptoms, without use of the classic tender point examination [111]. The majority of FM patients complain of sleep disturbance, emotional distress, and pronounced fatigue [1212]. FM represents the extreme end of the musculoskeletal pain spectrum in the general population. Several studies have demonstrated that this muscle pain is due to muscle ischemia, caused by decreased muscular blood flow and microcirculatory abnormality [1314]. Numerous recent studies emphasize the role of central nervous system (CNS) pain processing abnormalities in FM, including central sensitization, hyperalgesia, and inadequate pain inhibition [1516]. Therefore, the necessity of investigating pain modulation in the CNS continues to increase [17]. FM patients also suffer from numerous other chronic pain syndromes, which contribute to pain impulses and may serve to maintain central sensitization, including irritable bowel syndrome, temporomandibular disorder, migraine, low back pain, and peripheral coldness (e.g., Raynaud's phenomenon) [15].
Although the etiology of FM is not yet fully understood, the data suggest that FM may stem from autonomic nervous system dysfunction [18]; drugs that influence the autonomic system are being studied as potential treatments of FM [19]. Changes in autonomic nervous system function are known to accompany various diseases, including irritable bowel syndrome, chronic fatigue syndrome, migraine and other vasospastic symptoms [220]. Vasospastic symptoms, such as Raynaud's phenomenon and cold intolerance, occur in approximately 30% of patients with primary FM. NFC is a useful tool to evaluate Raynaud's phenomenon, by examining microcirculation abnormalities in other connective diseases [5]. A previous study showed that FM patients had fewer capillaries in the nailfold (p < 0.001), significantly more capillary dilatations (p < 0.05), irregular formations p < 0.01), and markedly reduced (p < 0.001) peripheral blood flow compared to healthy controls [4]. These data suggest that there are morphological abnormalities in microcirculation in FM, which can cause vasospastic symptoms.
We conducted this study to determine NFC patterns in FM, and their association with clinical features. A previous study indicated abnormalities in capillary numbers, dilatations and formations in FM on NFC. In addition to these parameters, we measured capillary dimension by calculating the number of pixels using the Adobe Photoshop software package [6]. In our study, FM patients had fewer capillaries, higher deletion scores and significantly decreased apical and capillary widths on NFC compared to healthy controls, which indicates that FM patients have abnormally decreased digital capillary diameter and density. Interestingly, there was no group difference in capillary dimension, which suggests that the length and tortuosity of capillaries in FM patients is increased to compensate for diminished microcirculation.
We observed that FM patients had altered capillary density and diameter in the digits; because FM is a disease characterized by unremarkable pathogenesis (and requires further study), diminished microcirculation on NFC may help to explain FM symptoms such as peripheral coldness, and may cause hormonal and biochemical abnormalities in FM pathogenesis that could lead to the development of advanced treatments for FM.
KEY MESSAGE
1. Diminished microcirculation and increased nailfold capillary tortuosity may explain fibromyalgia symptoms, such as peripheral coldness.
Acknowledgments
This research was supported by a fund from Soonchunhyang University.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.