Nododuodenal Fistula Caused by Tuberculosis
Article information
A 39-year-old woman presented to our hospital with upper abdominal pain. She had been taking anti-tuberculosis medications for 3 months because of pulmonary tuberculosis. Esophagogastroduodenoscopy showed a creamy discharge from an opening in the duodenal bulb (Fig. 1), and abdominal computed tomography with coronal reformatting showed that the lymph nodes had eroded the adjacent duodenum, resulting in a small oval collection of gas (Fig. 2). The continuous use of anti-tuberculosis medication resulted in complete healing of the duodenal fistula. Tuberculous lesions of the duodenal bulb may primarily affect the duodenum or produce compression because of the enlarged lymph nodes. The common complications of duodenal tuberculosis are fistulous communications with adjacent structures, perforation, and obstruction. Our case was a rare but interesting case that showed a creamy discharge from a nododuodenal fistula resulting from tuberculosis.
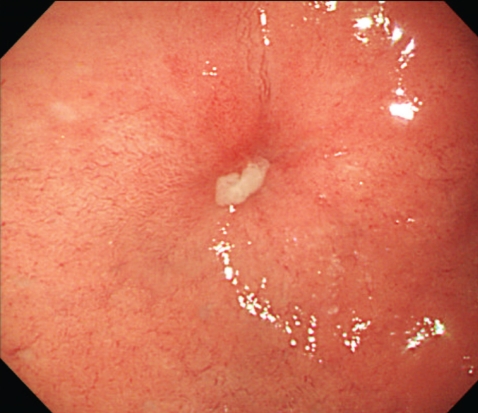
Esophagogastroduodenoscopy identified creamy discharges from an opening in the duodenal bulb.

Abdominal computed tomogaraphy with coronal reformatting shows that the lymph nodes eroded the adjacent duodenum, resulting in a small oval gas collection in the suprapancreatic lymph nodes with foci of low attenuation (arrow).
Notes
No potential conflict of interest relevant to this article was reported.