A Combination of Melphalan, Prednisone, and 50 mg Thalidomide Treatment in Non-Transplant-Candidate Patients with Newly Diagnosed Multiple Myeloma
Article information
Abstract
Background/Aims
The clinical efficacy and safety of a three-drug combination of melphalan, prednisone, and thalidomide were assessed in patients with multiple myeloma who were not candidates for high-dose therapy as a first-line treatment. Because the side effects of thalidomide at a dose of ≥ 100 mg daily can be a barrier to effective treatment for these patients, we evaluated the efficacy and safety of a reduced dose of thalidomide, 50 mg, for non-transplant candidates.
Methods
Twenty-one patients were treated in 4-week cycles, receiving 4 mg/m2 melphalan and 40 mg/m2 prednisone on days 1-7 and 50 mg thalidomide daily. The primary efficacy outcome was the overall response rate. Aspirin (100 mg daily) was also provided as prophylactic treatment for thromboembolism.
Results
The overall response rate was 57.1%; a complete response was seen in 23.8% of patients, a partial response in 33.3%, and stable disease in 9.5%. After a median follow-up time of 16.1 months, the median time to progression was 11.4 months (95% confidence interval, 2.1 to 20.6); the median overall survival was not reached. Grades 3 and 4 adverse events included infection (10%), peripheral neuropathy (5%), diarrhea (5%), thrombosis (10%), and loss of consciousness (10%). Two patients discontinued treatment due to loss of consciousness and neuropathy.
Conclusions
Low-dose thalidomide (50 mg) plus melphalan and prednisone is an effective combination drug therapy option for newly diagnosed myeloma patients who are ineligible for high-dose chemotherapy.
INTRODUCTION
Multiple myeloma accounts for approximately 10% of hematological malignancies and has increased in frequency due to aging of the general population [1]. Half of all multiple myeloma patients are older than 70 years of age, and 20% are older than 80 years of age [2]. In Korea, the incidence of multiple myeloma has increase steadily over the last 25 years [3], and the current incidence rate exceeds 1.0/100,000. Aging is an important factor that has contributed to the increase in the incidence of multiple myeloma in Korea [4].
Thalidomide has been successfully combined with corticosteroids and alkylating agents in the treatment of multiple myeloma. Palumbo et al. [5] showed that a combination of melphalan, prednisone, and thalidomide (MPT) showed a significant difference in progression-free survival compared with melphalan and prednisone alone (MP), but had no benefit for overall survival. Studies by the Intergroupe Francophone du Myelome (IFM), 01/01 trial [6] and Wijermans et al. [7] showed similar results. The IFM 99-06 trial reported a significant overall survival advantage for MPT compared with MP treatment [8]. These results indicated that the MPT combination can be considered an effective first-line treatment for elderly patients with multiple myeloma.
The optimal dose of thalidomide in an MPT regimen has yet to be determined. In two previous studies, the dose of thalidomide was 100 mg daily [5,6], and another study used a dose of 200 mg daily [7]. In the IFM 99-06 study, patients received a median dose of 200 mg/day [8]. However, these doses resulted in numerous adverse effects. Although toxic effects of MPT such as thromboembolism are manageable (e.g., low-dose aspirin for the prophylaxis of deep venous thromboembolism), a reduction in the dose of thalidomide as soon as symptoms appear is recommended. Thalidomide toxicity increases with the dose [9]. The side effects of thalidomide at a dose of ≥ 100 mg daily are barriers to effective treatment for patients who are not candidates for high-dose therapy as a first-line treatment. Therefore, we evaluated the efficacy and safety of a reduced dose of thalidomide, 50 mg daily, in an MPT regimen for non-transplant candidates.
METHODS
Patients
The study enrolled patients from seven clinical centers in Korea. Patients were previously untreated myeloma patients who were between the ages of 18 and 85 years, had measurable disease, a monoclonal (M) protein concentration of ≥ 1 g/dL or a urine M protein concentration of ≥ 400 mg/day, an expected survival time of ≥ 3 months, and a creatinine clearance rate of ≥ 20 mL/min. Exclusion criteria were presence of another cancer, psychiatric disease, or any grade 2 peripheral neuropathy. Abnormal cardiac function, preexisting pulmonary embolism, and abnormal liver function were not criteria for exclusion.
The study protocol was approved by the institutional review boards of each participating center. All patients gave written informed consent before entering the study, which was performed in accordance with the Declaration of Helsinki and the Korean Multiple Myeloma Working Party (KMMWP-KMM62).
Study design
This study was an open-label, non-randomized, clinical trial conducted at seven hospitals in Korea. The primary efficacy outcome was the overall response rate (ORR), classified as a complete response (CR), very good partial response (VGPR), or a partial response (PR). Secondary outcomes included time to disease progression (TTP), overall survival (OS), and toxicity. TTP was defined as the time from initiation of treatment to disease progression; deaths resulting from causes other than disease progression were censored. OS was defined as the time interval from initiation of treatment to death from any cause. Duration of response was defined as the period from the first observation of a PR to the date of disease progression; deaths resulting from causes other than progression were censored.
Treatment and dose modification
Treatment consisted of 4-week cycles of melphalan (4 mg/m2) and prednisone (40 mg/m2) on days 1-7, with 50 mg thalidomide given daily. Patients were also given 100 mg aspirin daily to prevent deep vein thromboembolism. Dose reduction of MPT was allowed after the first 4-week cycle. Treatment continued for six cycles or more, at the investigator's discretion, until disease progression, withdrawal of consent, or unacceptable treatment-related toxicity occurred. Melphalan and thalidomide could be withheld during cycle 1 for reasons of neutropenia or thrombocytopenia higher than grade 3. Patients with delayed recovery of hematologic toxicity (i.e., grade > 1 for more than 2 weeks) had a 25% dose reduction of melphalan.
Assessment of response and toxicity
Patient response was assessed using serum and urine M protein concentrations measured after cycle 2 and after every other cycle thereafter. Response to treatment, determined at the time of maximal response, was defined according to the European Group for Blood and Marrow Transplantation criteria [9]. Additional categories of near-complete response (nCR), defined by the absence of M protein after electrophoresis with positive immunofixation, and VGPR, defined by a > 90% reduction in M protein, were included. CR required confirmed disappearance of M protein in the serum and urine by immunofixation studies and < 5% plasma cells upon bone marrow examination. A PR was defined as a ≥ 50% reduction in serum M protein and a reduction in 24-hour urine M protein of ≥ 90% or to < 200 mg, plus no increase in the number or size of lytic bone lesions or any other evidence of disease progression. Progressive disease (PD) was defined as recurrence of disease after a CR or a > 25% increase in M protein from its lowest point. Patients who did not meet the criteria for CR, PR, or PD were classified as having stable disease. Adverse events were assessed during each cycle and graded according to the National Cancer Institute Common Toxicity Criteria, version 3.0 (NCI-CTC v3.0).
Statistical analysis
This study was initially planned using a grouped sequential design [10] with an expected risk reduction (RR) of 70% in the MPT arm compared with a 50% RR in the MP arm (refer to Appendix 1). However, after the first stage, investigators decided to terminate the study early for two reasons: lack of insurance coverage for thalidomide and delayed enrollment. All statistical analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). OS and TTP were estimated using the Kaplan-Meier method.
RESULTS
Patient characteristics
Twenty-one patients with newly diagnosed multiple myeloma, who were non-transplant candidates, were enrolled in our study between June 2006 and December 2008. Clinical characteristics of the cohort are summarized in Table 1. In brief, the median patient age was 70 years (range, 59 to 79), with three patients (14.3%) older than 75 years, and 47.6% of the patients were men. Six (28.6%) and 15 (71.4%) patients were classified as Durie-Salmon stages II and III, respectively.
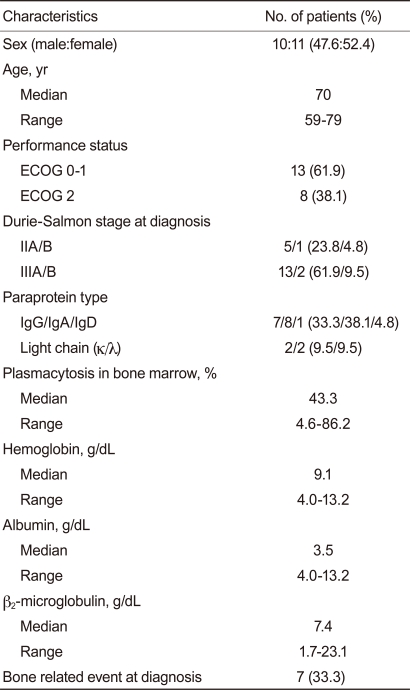
Patient characteristics (n = 21)
Response
A total of 21 patients received 92 cycles of MPT (median, 4 cycles; range, 1 to 12) (Table 2). Responses of three patients could not be evaluated because of death or loss to follow-up within two cycles of MPT therapy. Among 18 patients available for evaluation, five patients (23.8%) achieved a CR after two cycles of therapy, including two patients with an nCR, and six patients (33.3%) had a PR, including one patient with a VGPR, resulting in an ORR of 57.1%. The median duration of response was 5.5 months (range, 0.7 to 17.5).
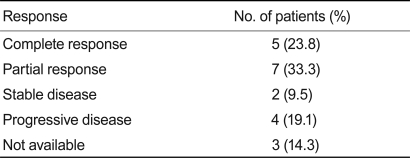
Response rates of patients after a combination of melphalan, prednisone, and thalidomide therapy (n = 21)
Survival
The median duration of follow-up was 16.1 months (range, 2.1 to 42.5). The median TTP was 11.4 months (95% confidence interval, 2.1 to 20.6); the median OS was not reached (Fig. 1).
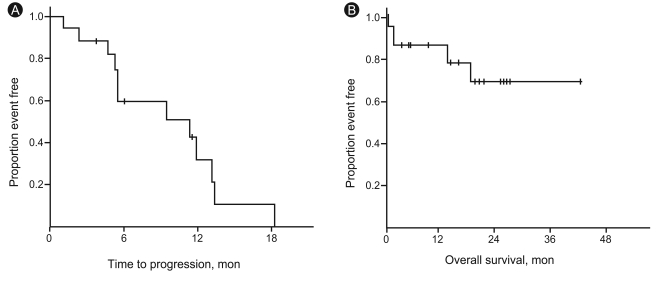
(A) Time to progression and (B) overall survival.
Toxicities
Twenty patients were assessed for toxicity from MPT. Hematologic and non-hematologic toxicities are shown in Table 3. Grades 3 and 4 hematologic toxicities included neutropenia (5%), thrombocytopenia (5%), and anemia (5%). Grades 3 and 4 non-hematologic toxicities were thromboembolism (10%), infection (10%), loss of consciousness (10%), and diarrhea (5%). Peripheral neuropathy was noted in 50% of patients, including 5% with grade 3 neuropathy. Fatigue, nausea, and hepatotoxicity of grades 1 and 2 were also reported during MPT therapy.
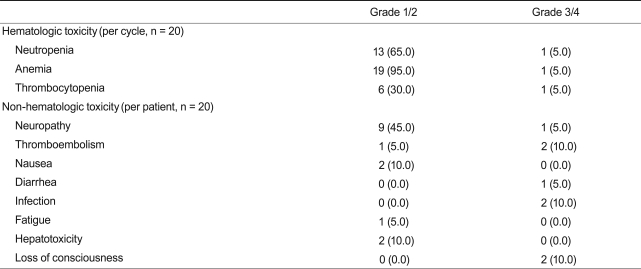
Adverse toxicity events after a combination of melphalan, prednisone, and thalidomide treatment
One patient (4.8%) died of an unknown cause after she had received one cycle of MPT. No autopsy was performed. One patient experienced loss of consciousness after he had received one cycle of chemotherapy. No specific abnormalities were found in this patient upon brain imaging, but it was decided that he would discontinue the MPT regimen. Another patient had grade 3 sensory neuropathy after he had been treated with four cycles of MPT. He achieved CR, and it was decided that he would discontinue MPT, as he did not want maintenance therapy.
DISCUSSION
High-dose chemotherapy (HDT) followed by autologous stem cell transplantation (ASCT) has improved the survival of both young [10] and elderly patients with multiple myeloma [11]. However, about half of patients with newly diagnosed multiple myeloma are over 70 years of age or have inadequate end-organ function, which are potential limitations for treatment with HDT and ASCT. The combination of melphalan and prednisone has been the standard treatment for such patients, but patient outcomes are less than satisfactory [12].
Recently, thalidomide used in combination with MP has become a first-line treatment regimen in non-transplant candidates and has resulted in superior outcomes in elderly patients compared with MP treatment alone [5-8]. Although MPT has shown promising results, the optimal dose of thalidomide has yet to be established. The Nordic group suggested that increasing the dose of thalidomide to 400 mg/day in very elderly patients could be associated with greater toxicity and more adverse outcomes [13]. Therefore, to reduce the adverse effects associated with thalidomide, the dose of thalidomide was decreased from 800 mg in the first trial to 100 mg, and more recently, to 50 mg/day [14-16]. The goal of clinicians is to use as low a dose of thalidomide as possible.
This study used 50 mg thalidomide plus MP and demonstrated a 57.1% ORR. In comparison, the IFM 01/01 trial, which included patients older than 75 years, showed a 62% ORR after MPT treatment [6]. Complete and partial response rates were 23.8% and 33.3% in this study and 7% and 41% in the IFM 01/01 trial, respectively. The median progression-free survival (PFS) time was 24.1 months in the IFM 01/01 trial, and the median time to progression was 11.4 months in this study. Our study showed similar response rates but shorter response durations than did the IFM 01/01 trial. The use of novel agents (thalidomide, bortezomib, lenalidomide) is also associated with high response rates, and recent trials showed that patients achieving CR had significantly longer PFS than patients achieving PR [17]. Although our study demonstrated a higher CR rate than the IFM 01/01 trial reported, the duration of response and survival were less satisfactory for our cohort. However, our definition of CR was different from that of the IFM 01/01 trial, as we included nCR patients, whereas the IFM 01/01 trial did not. Additionally, patients in the IFM 01/01 trial were treated for 12 cycles, whereas our patients were typically treated for six cycles. These differences might explain the apparent discrepancy between the studies in CR rate and survival.
With respect to the withdrawal rate from the IFM 01/01 trial, 48 patients (42.4%) discontinued treatment due to toxicities, whereas two patients (10%) discontinued treatment in our study. Additionally, the IFM 01/01 trial reported that 20% of patients required a dose reduction of thalidomide to 50 mg/day due to grades 1 and 2 peripheral neuropathy. Waage et al. [13] had similar results for a patient who was not eligible for HDT with ASCT. They demonstrated a 57% ORR and a median of 15 months PFS with MP and 200 or 400 mg of thalidomide. Fifty-nine patients (32.4%) discontinued thalidomide treatment due to toxicity. These data suggest that patients with multiple myeloma treated with 50 mg thalidomide had good compliance.
Venous thromboembolism (VTE) is a critical clinical condition manifesting as deep vein thrombosis and/or pulmonary embolism. Thalidomide treatment is associated with an increased risk of VTE, especially when used in combination with dexamethasone and/or chemotherapy. The risk is generally greatest in patients treated with thalidomide as a first-line therapy, as opposed to patients treated after relapse [18]. The percentage of thromboembolic events with thalidomide therapy in our study (10%) was higher than previously reported in Korean patients in general (3.9%) [19]. However, this incidence was lower than data from Western cohorts, which showed 6-17% incidences of VTE [5,6,8] after MPT treatment. Our study cohort included just 21 patients, which may have affected our interpretation of side effects.
The small number of patients enrolled in our study is a major limitation of this study. Despite the original study design, we decided to terminate this trial early for two reasons: absence of adequate insurance coverage of thalidomide and delayed enrollment of patients. Thalidomide is not covered by insurance for use as a first-line chemotherapy drug in Korea, but only as a secondary treatment after progression with first-line chemotherapy. Furthermore, patients with newly diagnosed multiple myeloma who were first treated with MP plus 50 mg thalidomide (MPT50) in our study, at high personal cost, could not use thalidomide combination therapy as a second-line chemotherapy option due to lack of insurance coverage. These challenges also resulted in delayed patient enrollment. Additionally, the availability of other new, active drugs (i.e., bortezomib and lenalidomide), which elicited good responses from patients not eligible for transplant [20,21], delayed enrollment of a sufficient number of patients. We evaluated the responses of 20 patients, 12 of whom responded to MPT50. According to the algorithm for enrollment (Appendix 1), our ideal cohort should have been 40 patients. Due to the various factors that prevented enrollment of a sufficient number of patients in a timely fashion, we decided to end this trial early.
In conclusion, our results suggest that MPT50 is an effective first-line treatment option for non-transplant-eligible patients with multiple myeloma, including elderly patients. To better identify the most appropriate patients for MPT50 therapy, however, additional large-scale prospective studies are needed.
Notes
No potential conflict of interest relevant to this article was reported.
Appendices
Appendix 1
Algorithm for patient enrollment, according to expected response

CR, complete response; PR, partial response.