Smoking Rather than Diet Deficiency is Related with Airway Obstruction in Korea
Article information
See Article on Page [Related article:] 132-139
Lung is an organ which contacts thousands of environmental toxins every day. Dietary factors such as antioxidant vitamins are known to have been implicated in the prevention of pulmonary emphysema [1-3]. To investigate the relationship between the dietary factor and the development of obstructive airway disease, Dr. Lee and colleagues analyzed Korean National Health and Nutrition Examination Survey (NHANES II), and found that only low protein intake was associated with obstructive airway disease among dietary factors, and non-dietary factors such as smoking, hypertension, and a low income were closely associated with airway obstruction.
The association between obstructive airway and dietary deficiency is already published. A study conducted in the Warsaw Ghetto during World War II revealed that incidence of emphysema was 13.5% in people who died of starvation [4]. Coxson et al. [5] also showed that severity of emphysema measured by computerized tomography was greater in an anorexic group. However, in Korea, obesity was more prevalent than malnutrition in NHANES II [6]. The proportion of low body mass index (BMI) was only 4.6%, while high BMI was seen in 30.6% (Fig. 1). Therefore, obesity rather than nutritional deficiency seems to be an important factor of health problem in general Korean population. In the other way, population with low income is more vulnerable to malnutrition. Thus, low income may cause low BMI, and this may be associated with obstructive airway disease. This presumption may be supported by subgroup analysis that low BMI population shows the close relationship between dietary deficiency and the development of obstructive airway disease in NHANES II.
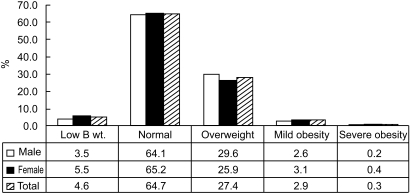
The proportion of obesity in Korean population according to sex. Definitions by body mass index (BMI): low body weight, < 18.5 kg/m2; normal, 18.5 to 24.9 kg/m2; overweight, 25.0 to 29.9 kg/m2; mild obesity, 30.0 to 34.9 kg/m2; severe obesity, > 35.0 kg/m2. B wt., body weight.
Smoking is a well known cause of chronic obstructive airway disease worldwide, and smoking cessation is the only effective way to ameliorate the speed of the lung volume reduction, to reduce the development of emphysema, and to prevent airway inflammation and carcinogenesis. Smoking was 5 times more risky to develop airway obstruction in Korean population. Moreover, smokers with hypertension had more than 7 times higher risk of airway obstruction than never-smokers without hypertension. Epidemiologic studies evaluating the risk of heart disease have consistently shown that reduced lung function is a major risk factor for cardiac death [7]. Therefore, smoking cessation should be the urgent target to prevent airway obstruction, hypertension and death in Korea.
Notes
No potential conflict of interest relevant to this article was reported.