Irinotecan, Continuous 5-Fluorouracil, and Low dose of Leucovorin (modified FOLFIRI) as First Line of Therapy in Recurrent or Metastatic Colorectal Cancer
Article information
Abstract
Background
Irinotecan, in combination with 5-fluorouracil (5-FU) and a high dose of leucovorin (LV), known as FOLFIRI regimen, has shown activity in recurrent or metastatic colorectal cancer. Therefore, we evaluated the efficacy and safety of irinotecan, 5-FU and a low dose of LV (modified FOLFIRI) as a first line of therapy for patients with relapsed or metastatic colorectal cancer.
Methods
Between January 2002 and October 2004, 44 patients with histologically confirmed recurrent or metastatic colorectal cancer were enrolled. The chemotherapy regimen schedule consisted of 180 mg/m2 of irinotecan being administered intravenously (i.v) on Day 1,400 mg/m2 of 5-FU via i.v bolus with 600 mg/m2 of continuous infusion for 22 hrs on both Day 1 and 2, and 20 mg/m2 of leucovorin on both Day 1 and 2, repeated every two weeks.
Results
The overall response rate was 47.8%. Of the 40 evaluated patients, one had CR (2.3%) and 20 had PR (46.5%). Toxicities were mild and easily manageable. Three patients experienced 23 episodes of Grade 3/4 leukopenia., Only one patient developed Grade 3/4 diarrhea. None experienced Grade 3/4 thrombocytopenia.
Conclusion
Modified FOLFIRI with a low dose of LV is an effective and tolerable regimen for patients with recurrent or metastatic colorectal cancer.
INTRODUCTION
Over the past 40 years, 5-fluorouracil (5-FU) and leucovorin (LV) have been the mainstays of chemotherapy drugs for advanced colorectal cancer. Recently, the combination of two new drugs, irinotecan or oxaliplatin, combined with 5-FU and LV, have demonstrated modest activity and improved survival as a first or second line of treatment. Irinotecan (CPT-11), a topoisomerase I inhibitor, was initially shown to have activity as a second line of therapy in patients with 5-FU resistant disease1). In recent phase III clinical trials, irinotecan plus a 5-FU/LV regimen improved both response and survival rates when compared with the control arm2, 3). However, the schedule and dose of irinotecan and 5-FU/LV have been fully modified in many trials, and an optimal protocol has not yet been determined.
As a third line of therapy for patients with metastatic colorectal cancer, a simplified bimonthly schedule of irinotecan with a high dose of 5-FU LV (FOLFIRI regimen) showed both activity and an acceptable level of toxicity in heavily treated patients4). As a first line of treatment, this regimen showed 31~56% response rates, without serious toxicity5-7).
In determining the optimal dose of 5-FU and LV, it was found that a high dose of 5-FU delivered a better response rate and longer response duration than a low dose of 5-FU. On the other hand, a low dose of LV was as effective and produced similar toxicities as a high dose of LV in combination with 5-FU. These results indicated that, when in combination with 5-FU, a low dose of LV is as effective as a high dose in the palliative management of patients with metastatic colorectal cancer8).
In the present study, we retrospectively evaluated the efficacy and safety of irinotecan, 5-FU and a low dose of LV (modified FOLFIRI regimen) every two weeks in relapsed or metastatic colorectal cancer.
MATERIALS AND METHODS
Patients
Patients included in the study were required to be 18~75 years old with a confirmed histologically, metastatic or recurrent colorectal cancer, and who had not received any prior chemotherapy. Adjuvant treatment, if administered, should have been completed at least six months before being enrolled. Other inclusion criteria were as follows: (i) a performance status of 0-2 on the Eastern Cooperative Oncology Group (ECOG); (ii) a bi-dimensionally measurable lesion, with a metastatic lesion or lymphadenopathy greater than 10 mm; (iii) an adequate bone marrow reserve (WBC count >4,000/µL, platelet count >100,000/µL); and (iv) a normal cardiac function. (v) normal renal function (serum creatinine <1.5 times the upper normal limit (UNL)); (vi) an adequate hepatic function (AST and ALT <2.5 times UNL and total bilirubin <1.5 times UNL; patients with obstructive jaundice should have undertaken internal or external biliary drainage before enrollment); and (vii) an estimated life expectancy of at least 12 weeks at the time of enrollment. All approved patients or legal representatives signed informed consent forms before treatment began.
Treatment schedule
All patients received chemotherapy under the following schedule: 180 mg/m2 of irinotecan intravenously (i.v) on Day 1, 400 mg/m2 of 5-FU via i.v bolus with 600 mg/m2 of continuous infusion for 22 hrs on Day 1 and 2, and 20 mg/m2 of leucovorin on Day 1 and 2, every two weeks. Treatment was continued until the progressive disease, unacceptable toxicity, or withdrawal of the patients' consent.
Dose modification
Prior to each treatment, we recorded the patient's history and performed physical examinations, CBC (complete blood counts), blood chemistry, and conducted a urine analysis. If the absolute neutrophil count was less than 1,500/µL or the platelet count was less than 100,000/µL, treatment was delayed for one week or until myelosuppression was resolved. If a patient was not fully recovered after seven days, the dose was reduced by 25%. If Grade 3/4 non-hematologic toxicity developed, the dose was decreased by 25%. If there was a second episode of Grade 3/4 non-hematologic toxicity, treatment was stopped.
Assessment of response and toxicity
Physical examinations, peripheral blood count, blood chemistry, and chest X-ray were performed during each patient visit. CT scans were performed at the baseline and after four treatment courses. Response to treatment was assessed according to World Health Organization (WHO) criteria. Before each cycle, patients were assessed for toxicity according to the National Cancer Institute common toxicity criteria.
Statistics
Time to progression (TTP) was defined from the first day of chemotherapy to the day of confirmed progression. Overall survival (OS) was calculated from the first day of chemotherapy to death or final follow-up. All data were analyzed using the Kaplan-Meier method using the SPSS program (version 11.0).
RESULTS
Clinical characteristics
A total of 44 patients (32 men and 12 women) diagnosed between January 2002 and October 2004 at Kangnam St. Mary's Hospital and St. Mary's Hospital were enrolled in this study. The median age was 58 years (range: 27-72 years). Twenty-two patients had recurrent cancer after curative surgery, while 22 patients had metastatic diseases at the initial diagnosis. Nineteen patients had received adjuvant treatment with 5-FU and LV or 5-FU chemoradiation. At baseline, all patients had and ECOG performance between 0 and 2. Patients' characteristics are summarized in Table 1. Most of the patients received chemotherapy with oxaliplatin containing a regimen after diagnosis of progressive disease.
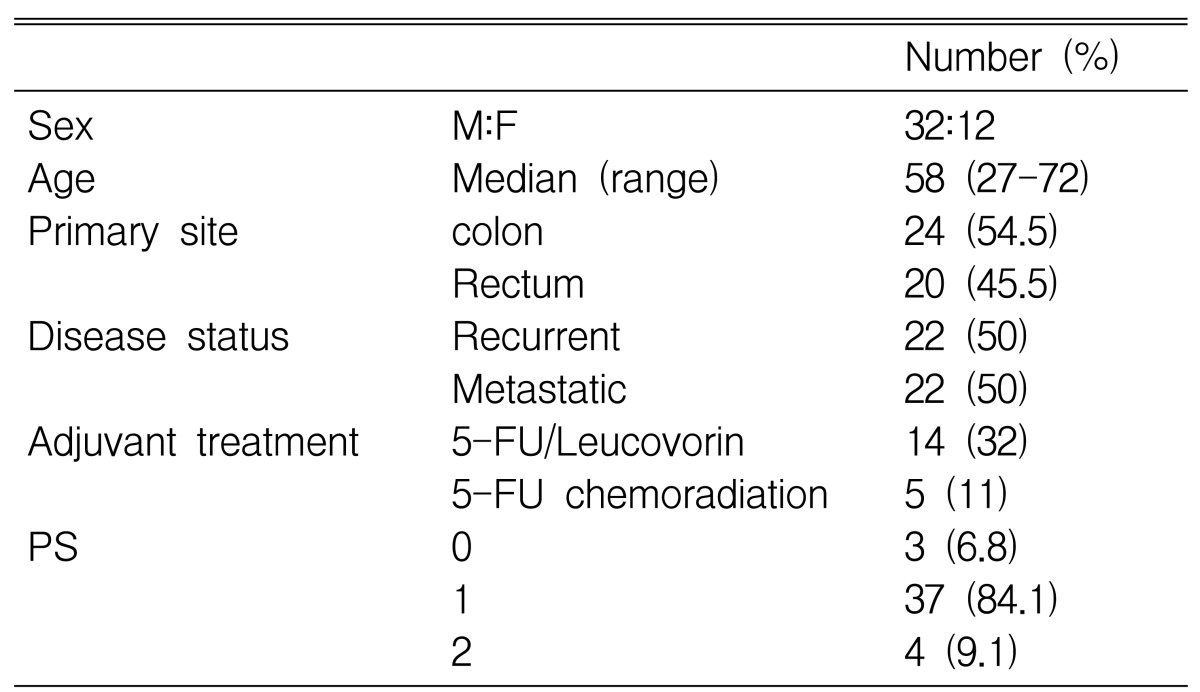
Baseline patients characteristics
Treatment efficacy
Of the 44 patients enrolled, 4 patients were lost to follow-up after the first cycle. One patient refused all anti-cancer therapy, and two patients could not withstand the irinotecan-containing chemotherapy. An additional patient, who experienced Grade 4 neutropenic infection during the 1st chemotherapy cycle, changed their chemotherapy regimen.
The total number of cycles was 288, and the median number of cycles was six (range, 1-16). The overall response rate was 47.8% (95% Confidence interval; 32.5~63.2%) (Table 2). Of the 44 patients, one had CR (2.3%), while 20 had PR (45.5%). Of the 40 evaluated patients, the response rate was 52.5% (95% Confidence interval; 37.2~67.8%). There was no significant difference in response rates associated with previous chemotherapy history (Table 3) (p=0.054). The median follow-up for surviving patients was 53 weeks (23-121 weeks). The median time to progression was 23 weeks (7-57 weeks) while median survival was 47 weeks (18-121 weeks) (Figure 1).
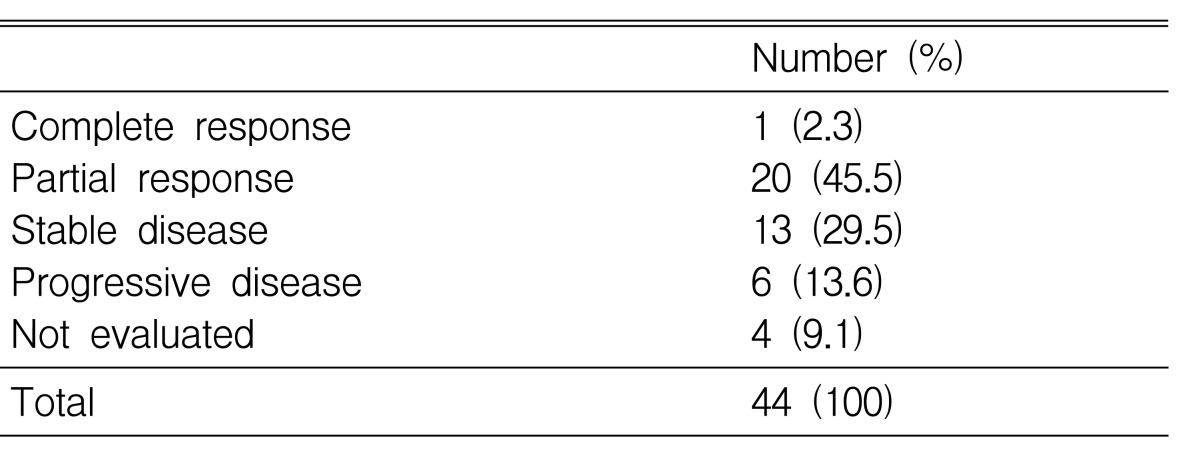
Response to chemotherapy

Response rate according to previous chemotherapy history
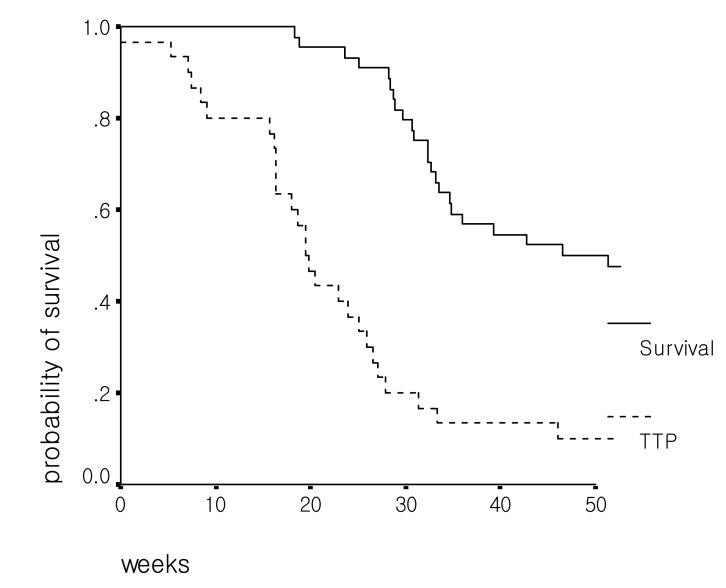
Time to progression & Overall survival
Toxicity
A total of 288 cycles for 44 patients were evaluated for toxicity, and the toxicity incidence is summarized in Table 4. One patient required a 25% dose reduction due to delayed bone marrow suppression, and two patients required a delay of treatment for one week due to non-recovery from bone marrow suppression. Three patients experienced a total of 23 episodes of Grade 3/4 leukopenia, but no Grade 3/4 thrombocytopenia was observed (Table 4). Two patients experienced Grade 3/4 neutropenic infections without septic shock. No treatment-related deaths occurred.
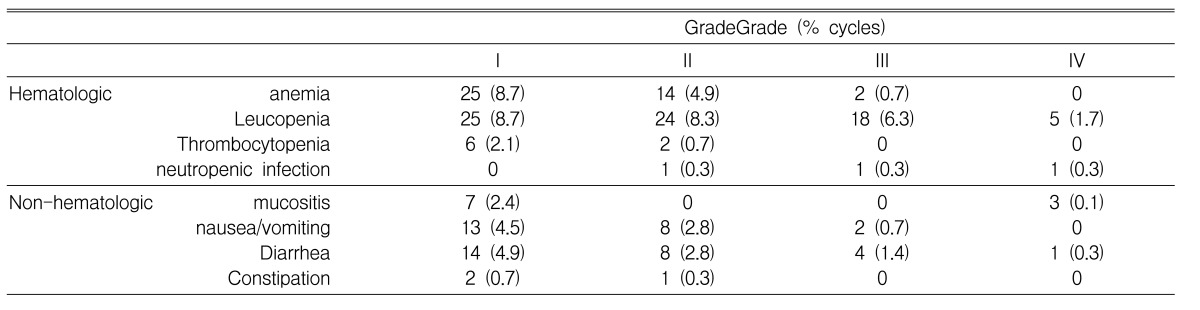
Toxicity
The most common non-hematologic toxicities were diarrhea, nausea and vomiting. But only one patient developed Grade 3/4 diarrhea, and one patient developed Grade 3 vomiting. Three episodes of Grade 4 mucositis were observed in one patient. No treatment-related deaths occurred during any of the chemotherapy cycles.
DISCUSSION
FOLFIRI, (a combination of irinotecan, 5-FU and LV), has been recommended as a standard treatment for advanced colorectal cancer, having shown response rates of 39.8~56% as a first line of treatment2, 3, 5). However, a clinical trial using this regimen in Germany, subsequently showed a response rate of only 31%, which may have been due to a higher percentage of patients with two or more metastatic sites, and hence a larger tumor6). The poorer outcome in this trial may have been due to the inclusion of a greater percentage of patients with rectal cancer (34%), or to the enrollment of patients previously treated with 5-FU and LV (14%). In our trial, using a modified FOLFIRI regimen, 45.5% of the patients had rectal cancer and 43% had previous treatment with 5-FU chemotherapy regimen. We recorded a response rate of 47.8%, suggesting that the lower response rate in the German trial was not due to the inclusion of patients with rectal cancer or those previously treated with 5-FU or LV. Rather, other factors, such as molecular markers, may be more important in predicting responses to the FOLFIRI regimen.
Three clinical trials in South Korea have tested the combination of irinotecan, 5-FU and LV for advanced colorectal cancers. In a study using a high dose of LV, 8 out of 20 evaluated patients attained partial response (40%) and the median overall survival was 17.3 months9). Using 150 mg/m2 of irinotecan and a low dose of LV (20 mg/m2) in patients with metastatic colorectal cancer as a second line of treatment, the response and median survival rates were lower (20% and 39.6 weeks), respectively10).
This lower response rate may have been due to the use of this chemotherapy regimen as a second line of treatment or to the lower dose of irinotecan. However, a lower response rate (27.3%) was observed in patients with metastatic colorectal cancer using a regimen identical to ours, but with fewer treatment cycles11). Although we found that FOLFIRI with a low dose of LV, achieved a response rate comparable to that of the previous study (47.8% vs. 40%), the median overall survival time was somewhat shorter (11 months vs. 17-21 months). This may well have been due to the shorter follow-up period for surviving patients (median 13.3 months), suggesting that the median overall survival time should be reevaluated after a long-term follow-up.
The most common toxicities associated with irinotecan are neutropenia, anemia, delayed diarrhea, and fatigue. Since irinotecan was initially associated with high death rates12), its use has been modified to exclude patients who have a performance status 2 - at high risk for adverse events. In fact, Grade 3/4 gastrointestinal even, especially diarrhea, was the most common serious problem with an incidence of 22~45%13-16). Thus, the monitoring of patients for gastrointestinal (e.g. diarrhea, nausea, abdominal cramping) and thromboembolic events during treatment is essential. If fever associated with neutropenia develops, prompt supportive care, including early use of oral fluoroquinolone, are needed17).
However, in our study, incidence of Grade 3/4 delayed diarrhea was only 1.7%. We had instructed all patients in this trial to take anti-diarrhea agents if they had diarrhea more than five times a day (but almost patients did not take medication). In other trials of irinotecan in South Korea, Grade 3/4 delayed diarrhea was not common, having an incidence of 1.2~6.7%9-11), unlike in Western countries. We suggest that this may be due to ethnic differences, although we could not determine whether any medications to prevent delayed diarrhea were administered in the other South Korean clinical trials. We found that other non-hematologic toxicities were manageable and reversible, and overall, patients tolerated this regimen.
In summary, irinotecan, 5-FU and a low dose of LV may be as effective as irinotecan, 5-FU and a high dose of LV, and considerably tolerable for patients with recurrent or metastatic colorectal cancer as a first line of treatment.