Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in a Young Patient with Long Term Kawasaki Disease
Article information
Abstract
Kawasaki Disease (KD) is an acute, febrile, multisystem disease of children. More severe complications in 15~25% of cases include, the development of coronary aneurysms, ischemic heart disease, and sudden cardiac death. The standard treatment for significant coronary artery stenosis has generally been aortocoronary bypass surgery, although percutaneous transluminal coronary angioplasty (PTCA) has been described in a small number of patients. This report describes a 14 year old boy with a history of KD who developed multiple coronary aneurysms and stenosis. We performed PTCA, which was successful in relieving the stenosis of the left circumflex artery.
INTRODUCTION
Kawasaki Disease, first described in 1967, is a serious childhood illness characterized by high fever, conjunctivitis, erythema of oral mucosa and pharynx, a "strawberry" tongue, diffuse inflammation of both hands and often feet, polymorphous desquamative rash, and acute non-purulent cervical lymphadenopathy. In the absence of laboratory measurements, KD is diagnosed when five of the six symptoms are identified. Alternatively, the disease may also be diagnosed if coronary aneurysms are found in addition to four of the major symptoms. In some patients, the long-term sequelae of vasculitis occurring in KD results in coronary artery aneurysms, thrombotic occlusions, progression to ischemic heart disease, and/or premature arteriosclerosis5-7). Approximately 4% of coronary aneurysms subsequently develop stenotic lesions, half of which occur within 2 years of the onset of KD6). The standard treatment for significant coronary artery stenosis has generally been aortocoronary bypass surgery1,2), although PTCA has been described in a small number of patients3,4). We describe here a 14 year old male with KD who developed stenosis of the coronary arteries, which was successfully managed with PTCA.
CASE REPORT
A 14-year-old boy was admitted to our institution for elective PTCA to relieve stenosis of the coronary arteries. At 4 years and 7 months of age, the patient presented to our institution with typical signs and symptoms of KD (persistent fever up to 39℃ for 10 days accompanied with conjunctival injection and a strawberry tongue). Consequently, the patient received intravenous gamma globulin and aspirin, which resulted in a prompt resolution of the fever and improvement of symptoms. Two-dimensional echocardiography performed during the acute phase of the illness demonstrated fusiform aneurysms of the right coronary artery (RCA) (10 mm in diameter), left anterior descending (LAD) branch (7 mm), and left circumflex (3.7 mm), as well as dilatation of the left main coronary artery (LMCA) (4 mm). However, there was normal systolic ventricular function without regional wall motion abnormalities. The patient was given low-dose aspirin and discharged from the institution. After discharge the patient was free of symptoms. An echocardiogram performed 15 months after the onset of illness demonstrated mildly improved fusiform aneurysms of the RCA (8.4 mm) and LAD (5 mm), as well as improved dilatation of LMCA (3.4 mm). However, there was no change in the left circumflex lesion. The patient was continued on a therapy of low-dose aspirin and remained asymptomatic. A 24 hour Holter monitor at 20 months, 40 months, and 68 months after presentation indicated normal heart rhythm with no evidence of ischemia. A treadmill test performed 9 years after presentation revealed no arrhythmias or ischemic changes. Nine years and 5 months after disease onset, selective coronary angiography revealed two saccular aneurysms in the proximal portion of the LAD, and in the proximal portion of the RCA as well as stenosis (minimal lesion in the proximal portion of the LAD, discrete lesion in the left circumflex, and total obstruction in the RCA with collateral arteries supplying blood to the distal portion of the RCA.)(Figure 1). The patient retrospectively reported symptoms of intermittent chest discomfort for 5 months prior to catheterization. On admission, his blood pressure was 120/80 mmHg. His heart rhythm was regular and his heart rate was 76 bpm. The patient looked well and his physical examination and laboratory results did not reveal any abnormalities. Accordingly PTCA was performed at 9 years and 6 months after the onset of illness. The procedure employed a 3.5 mm balloon catheter in the stenotic lesion of the proximal portion of the left circumflex. The balloon was then inflated with diluted contrast medium to a pressure of 10 atm. The area of stenosis was 80% before PTCA and there was no residual stenosis after PTCA (Figure 2). An intravascular ultrasound (IVUS) study was performed immediately after PTCA. The IVUS imaging revealed a calcified lesion and atheroma at the site of the left circumflex coronary artery (Figure 3). The patient tolerated the procedure well with no electrocardiographic changes. He was discharged home on aspirin, ticlopidine, and isosorbide dinitrate. To date, he has been well. Currently, the patient is following a regimen of low-dose aspirin.

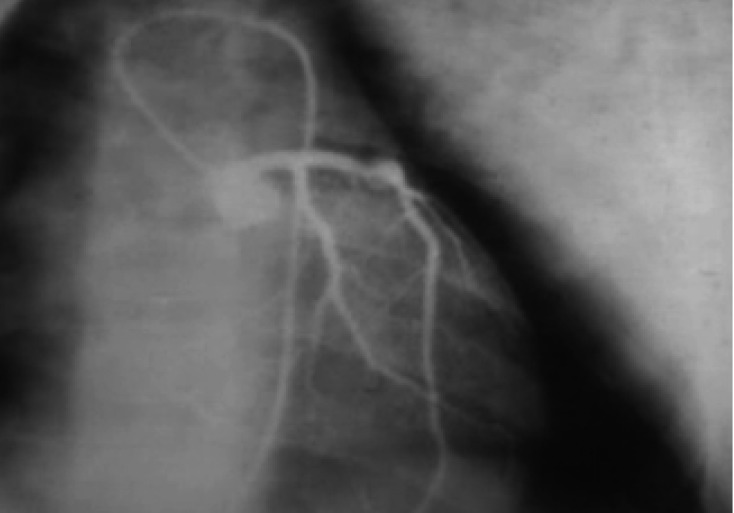
Left coronary angiogram with 80% stenosis on the proximal portion of the left circumflex (arrow).
Left circumflex stenosis improved from 80% to <25% after PTCA.

IVUS imaging at the left circumflex coronary artery site showed calcification (arrow).
DISCUSSION
Kawasaki Disease is an acute febrile illness occurring most often in infants and children. Fifteen to twenty percent of cases develop more severe complications including coronary aneurysms, ischemic cardiac disease, and sudden cardiac death. US epidemiologic studies of KD demonstrate the peak incidence of disease to be at 18 to 24 months of age, with children ≤5 years of age accounting for approximately 80% to 85% of cases. Surveys conducted in the study indicate that the male-to-female ratio is 1.3-1.5:1 in KD, whereas the male-to-female ratio is 4:1 in their study of the hemodynamic and coronary angiographic findings in children with KD with obstructive coronary lesions8).
The major long-term concerns of KD are the development of coronary artery lesions that may manifest as aneurismal lesions, thrombotic occlusions with progression to ischemic heart disease, and the development of premature arteriosclerosis5-7). Currently, with appropriate medical management (immunoglobulins and salicylates), about 4% of children with KD eventually develop ischemic heart disease, which is often associated with calcified stenosis during long-term follow up3,6,9). Since the disease was first described by Kawasaki in 1967, the mortality rate has decreased attributable, in large part, to the development of advanced diagnostic methods and treatment6). However, coronary artery aneurysm, a serious complication of KD, has remained a leading cause of acquired heart disease in children10). Therefore, the prognosis of KD correlates with the degree of coronary involvement. Kato and colleagues3) have reported the results of serial coronary angiography to clarify the fate of coronary aneurysms. Serial angiographic follow-up of KD patients has indicated that approximately 50% of 42 patients with coronary artery abnormalities showed resolution 5 to 18 months later, with giant aneurysms (defined as ≥8 mm in diameter) the least likely to regress and most likely to progress to stenosis8). The regression in coronary aneurysms was recognized within one or two years after onset; however, half of the patients with regressed coronary aneurysms continued to demonstrate a dense or bright echo in the coronary artery wall on a 2D-echocardiography6). The mechanism of coronary artery stenosis in KD is uncertain. One possibility is acute occlusion by massive thrombus formation in the coronary aneurysm, which occurs mostly in acute or subacute stages of illness. Another mechanism of coronary artery stenosis in KD may be the progression of marked thickening of the intima often associated with calcification, which is similar to an arteriosclerotic lesion11,12). The risk factors for progression to ischemic heart disease are giant aneurysm (diameter of more than 8 mm), a saccular aneurysm shape, prolonged fever for more than 21 days, and age at onset of less than 2 years13).
Interventions such as PTCA, atherectomy, or stent implantation are now common treatments for adults with coronary artery disease14,15). However the use of these treatments is limited in KD4). In particular, PTCA is not as effective in KD patients as in others because the stenotic lesions in long-term KD are stiff and often associated with calcification. Aortocoronary bypass surgery is the standard therapy for severe stenosis of coronary arteries with lesions that form as a result of KD1,2,16-18). Bypass surgery is indicated in cases with multiple vessel lesions, cases with severe valvular disease, and cases with severe left ventricular dysfunction19). The long-term patency of bypass grafts is satisfactory in older patients but remains unsatisfactory in young children with KD. Therefore, PTCA should be considered in young children to postpone bypass surgery until patients are of sufficient age and size, so that the bypass grafts are likely to maintain satisfactory long-term patency. Recent advances in intravascular ultrasound (IVUS) imaging have allowed pathological evaluation of the vascular wall structure of coronary stenosis12,20). Recently Ino and colleagues4) reported that the only predictor of successful PTCA seemed to be the elapsed time from the onset of KD to the performance of PTCA: PTCA performed within 6 to 8 years after onset of the disease is more likely to lead to successful dilatation, which means that stenotic lesions may develop arteriosclerotic changes in the long term. Factors such as age at onset, lesion site, sex, clinical symptoms, and presence or absence of a perfusion defect on a 201Thallium scintiscan did not appear to affect outcome of PTCA.
Our successful attempt may indicate that this procedure should be considered early in subclinical stenosis to prevent ischemic cardiac damage. We suggest that PTCA may successfully dilate stenotic coronary arteries that have relatively soft intima with only localized mild calcification. IVUS is useful in the assessment of wall morphology and tissue characterization of the pathological coronary artery as well as in the selection of the best device for interventional treatment. A catheter intervention for coronary artery stenotic lesions in KD demonstrated significant therapeutic effects in the short term. Intervention with a catheter is a promising therapeutic strategy in the management of coronary stenosis caused by KD. However, the long-term efficacy of a catheter intervention for KD is unclear. To verify these findings, more long-term follow-up studies are needed. Care should be paid to avoid acute coronary arterial complications and the development of new coronary aneurysms. Based on the successful of PTCA reported here, we recommend that the procedure should be considered early in subclinical stenosis to prevent ischemic cardiac damage.