Percutaneous Fine Needle Aspiration Biopsy of Pancreatic Cancer Guided by Ultrasonography
Article information
Abstract
Fine needle aspiration biopsy guided by ultrasonography was performed in 39 patients with pancreatic cancer to evaluate the value of the technique for establishing a proved histologic diagnosis. Aspirated material suitable for cytologic evaluation of smear preparation was obtained from 33 patients(84.6%). Among the 33 patients, cytologic diagnosis of pancreatic cancer was possible in 28 patients(84.9%). There was mild abdominal pain only in one patient(2.6%). In conclusion, percutaneous fine needle aspiration biopsy guided by ultrasonography proved to be a safe and useful method for histologic diagnosis of pancreatic cancer.
INTRODUCTION
Despite refined roentgenographic, endoscopic and isotopic techniques, the diagnosis of pancreatic lesions still presents a great problem in many instances1).
Recently, with rapid development of imaging diagnostic modalities such as ultrasonography and computed tomography, it has been possible to obtain information about the pancreas and to perform percutaneous fine needle aspiration biopsy of pancreatic cancer guided by these techniques.
We wish to present our experience with percutaneous fine needle aspiration biopsy guided by ultrasonography in a total of 39 patients with pancreatic cancer and to evaluate the value of the technique for establishing a proved histologic diagnosis, avoiding operative intervention and facilitating treatment planning.
MATERIALS AND METHODS
Thirty-nine patients with pancreatic cancer were studied from March 1984 to July 1987. The age range of the 39 patients was 29 to 72 years(mean 54 years). There were 25 men and 14 women (Table 1). Of the 39 patients, the pancreatic cancer was diagnosed by operation in 7 patients, three diagnostic methods (computed tomography, ultrasonography and ERCP) in 5 patients, two diagnostic methods such as ultrasonography and computed tomography in 10 patients, ultrasonography and ERCP in 6 patients and ultrasonography in 11 patients with clinical grounds.

Age and Sex Distribution
Ultrasound investigations were performed in the fasting supine patients by means of a real-time scanning technique (Aloka echo camera LS model SSD-280 with a real-time linear-array scanner having a frequency of 3.5MHz). The cancer of the pancreas was delineated, providing a three-dimensional presentation of its sonoanatomy. Special care was taken to identify the major abdominal vessels and the adjacent viscera. Whenever possible, biopsy access routes representing the shortest distance between the skin and the target tumor were selected. The distance between the skin and the center of the target volume was measured on the ultrasonic display and transposed to the needle shaft with a sterile needle stop. The angle of the needle path (parallel to the ultrasonic beam) was indicated by the position of the transducer. We selected a pathway transversing the stomach. However, penetration of the colon was avoided to prevent bacterial spread.
Biopsies were performed using commercially available Chiba needles with a removable inner stylet and an outer diameter of 23 gauge. Local anesthesia with 2% procaine was utilized in all patients. The needle and syringe were heparinized before use by wetting the whole inner surface of the syringe with a small amount of sodium heparin. During suspended respiration, the needle was advanced into the area of interest. A variation in resistance was felt in a significant number of patients when the needle entered the tumor mass. When the needle tip had been introduced into the target volume, the mandrel was withdrawn and a special suction device equipped with a 20ml plastic syringe flushed with heparin was attached. While the patient was asked to stop breathing, the needle was quickly moved back and forth several times while applying aspiration to the mass. Suction should be discontinued before removal of the needle to prevent aspiration of neighboring tissue into the syringe or spillage of tumor cells along the needle track.
Two or three needle passes assured sufficient material. The aspirated material was smeared on glass slides, immediately fixed in 95% alcohol and stained by the Papanicolaou method, and collected on the filter paper in preparation for cell block. The results of cytology were reported as material insufficiency, or positive, suspicious or negative for cancer.
RESULTS
The symptoms and signs of the patients with pancreatic cancer (39 patients) were abdominal pain (35 patients, 81.7%), weight loss (20 patients, 51.3%), anorexia (13 patients, 33.3%), back pain (13 patients, 33.3%), jaundice (10 patients, 25.6%), dyspepsia (7 patients, 17.9%), palpable mass (5 patients, 12.8%) and bowel habit change (2 patients, 5.1%) (Table 2). Of the 39 patients, aspirated material suitable for cytologic evaluation of smear preparations was obtained from 33 patients (84.6%). Among the 33 patients, cytologic diagnosis was positive in 26 patients (78.8%), suspicious in 2 patients (6.1%) and negative in 5 patients (15.1%). There was mild abdominal pain only in one patient (2.6%) (Table 3).

Symptoms and Signs in Patients with Pancreatic cancer (n = 39)

Results of Fine Needle Aspiration Cytology in Patients with Pancreatic Cancer (n = 39)
All 39 patients were divided into three groups according to the size of the tumor such as group A (2.0≤ and <4.0cm, 22 patients), group B (4.0≤ and <6.0cm, 12 patients) and group C(≥6.0cm, 5 patients). The aspirated material was insufficient for cytologic evaluation in 6 patients (4 patients in group A and 2 patients in group B). Of the remaining 18 patients in group A, the cytologic diagnosis was positive in 15 patients and negative in 3 patients. Of the remaining 10 patients in group B, the cytologic diagnosis was positive in 7 patients, suspicious in 2 patients and negative in 1 patient and of the 5 patients in group C, the cytologic diagnosis was positive in 4 patients and negative in 1 patient (Table 4).
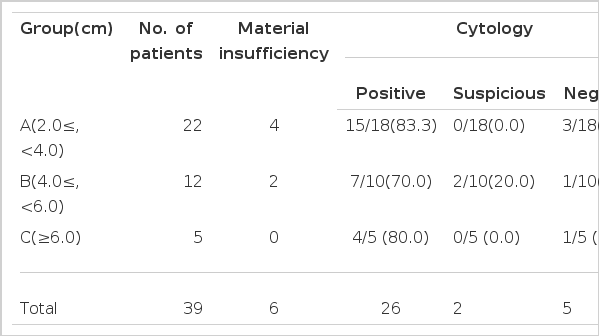
Results of Fine Needle Aspiration Cytology According to the Size of the Pancreatic Cancer
The cancer of the pancreas was located in the head (21 patients), the body (9 patients), and the tail (6 patients) portions of the pancreas and diffusely in 3 patients. The aspirated material for cytologic evaluation was insufficient in 6 patients (head:4, body and tail: 1 and respectively). The cytologic diagnosis was positive in 26 patients (head:12, body:8, tail:4 and diffuse:2), suspicious in 2 patients (head and tail:1 each respectively) and negative in 5 patients (head:4 and diffuse:1) (Table 5).
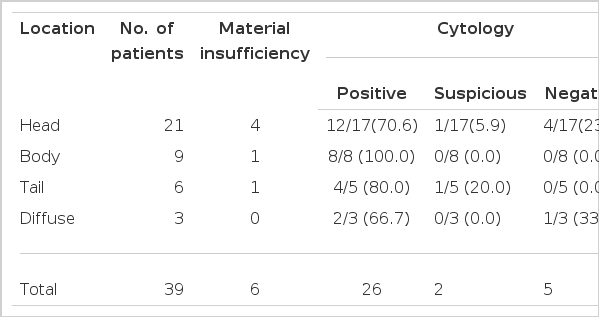
Results of Fine Needle Aspiration Cytology According to the Location of the Pancreatic Cancer
DISCUSSION
The widespread acceptance of thin-needle (21–23 gauge) aspiration biopsy for cytodiangosis of deep malignant tumors is due to the high yield of positive tissue samples as well as the low risk of serious complications2).
With recent improvements in localizing methods, the availability of thin needles for aspiration and the increased sophistication of the cytologic technique, the use of aspiration biopsies has been extended to that of mass lesions of the pancreas and other abdominal structures1,3–5).
Aspiration biopsy offers an approach to pancreatic cancer which is distinct from histology or tissue biopsy. The smaller outer diameter of the aspiration needle results in a cross-sectional area 5 to 13 times less than that of tissue biopsy needles. It is this difference that permits uncomplicated passage of the fine needle through the liver, stomach or bowel on the way to the pancreas6).
The major technical problem is localization of the lesion and this has been achieved by biopsy during angiography with test injections of contrast material into appropriate arteries under fluoroscopic control5,7), during ultrasonography using a special biopsy transducer1,4), with computed tomography to image the position of the biopsy needle8) and following ERCP9). Among them ultrasonography is well adapted to biopsy technique since the lesion can be quickly and accurately localized in any plane1,10).
Success with the fine needle aspiration biopsy technique requires an experienced and skilled cytopathologist. Also critical to a high yield is proper handling of the cytologic material11). The most recent data indicate a diagnostic accuracy between 80% and 100%. False-negative rates of 3% to 20% have been encountered, but false-positive results are virtually nonexistent1,3,5,7,9,12–14). In this study, the diagnostic accuracy (84.9%) was slightly lower than that of other reports. There was no significant difference of diagnostic accuracy according to the size of the cancer. However, pancreatic cancer located in the body showed a higher rate of diagnostic accuracy than the other portions.
Lack of diagnostic cytologic material may be related to necrotic and/or scirrhous areas in the tumor11). The reported falsepositive frozen section diagnoses have not occurred with fine needle aspiration4,6,7,15). In this study, aspirated material for cytologic examination was insufficient in 6 patients (15.4%), especially in patients having a small cancer size (2.0–4.0cm; 4 patients and 4.0–6.0cm; 2 patients).
Goldstein et al11) performed fine needle biopsy of the pancreas in 4 dogs and on subsequent laparatomy found little or no evidence of the needle punctures. Focal serosal bleeding is occasionally noted without evidence of perforation. Coel and Niwayama16) performed biopsies on 16 pigs without clinically apparent complication, although histologic examination of one of the specimens demonstrated a small are of focal hemorrage. There were reports of complications such as intestinal bleeding4), fatal necrotizing pancreatitis17) and hematoma3). In this study, mild abdominal pain was noted only in one patient (2.6%).
Seeding of malignant cells along the needle track is a recognized risk of paracentesis and thoracentesis for malignant effusions in carcinoma of the breast and ovary. Experimentally, Engzell et al.18) were unable to demonstrate release of tumor cells after thin-needle aspiration of transplanted malignant lymph nodes in rabbits. Reports of thousands of fine needle aspiration biopsies have generated a few reported cases of seeding of the skin at the aspiration site2,19–22). In addition, the theoretical possibility of hematogenous metastases from cells dislodged during aspiration has not been supported by clinical studies23–25). However, with fine needle aspiration biopsy, there has been no evidence of dissemination of cancer in a large series of patients with different tumor types of various organs19). In patients of this study, there was no seeding of malignant cells during the follow-up periods until now.
In conclusion, ultrasound-guided fine needle aspiration biopsy is considered to be a safe and useful method for histologic diagnosis of pancreatic cancer.