Changes of Peripheral T Lymphocyte Subsets Following Treatment in Patients with Bronchogenic Carcinoma
Article information
Abstract
We evaluated the changes of peripheral leukocyte counts, lymphocyte counts, and percentage of lymphocytes and T cell subsets (OKT4(%), OKT8(%) and OKT4/OKT8) in 49 untreated lung cancer patients of whom 23 were followed up after therapy (8 pulmonary resection, 15 chemotherapy). Total WBC counts were significantly increased in stage I or II compared to controls and were decreased after operation.
Total counts and percentage of lymphocytes were decreased (esp. stage III NSCLC, SCLC esp. ED, squamous) and were persistently decreased after treatment in nonresponders. OKT8(%) was decreased (esp. SCLC, squamous, adenocarcinoma, all stages of NSCLC, and ED of SCLC) and was persistently decreased in stage III after treatment.
The OKT4/OKT8 ratio was increased (esp. adenocarcinoma and stage III NSCLC) and returned to the normal range after treatment.
In nonresponders, total lymphocyte counts were decreased before treatment compared to responders and persistently decreased before and after treatment compared to controls, and OKT8(%) was persistently decreased after treatment compared to controls.
In conclusion, immunoabnormalities in patients with lung cancer might be improved following treatment.
INTRODUCTION
Patients with lung cancer often display impaired immunity,1–10) including low counts of T-lymphocytes, and these impairments have been postulated to be significant in the development and progression of lung cancer, and the nutritional status of patients has been contributed to immunologic abnormalities4).
Recently, Wesselius et al.4) have reported on lymphocyte subsets in patients with untreated lung cancer, and we also have reported on T lymphocyte subsets in patients with untreated lung cancer.10) But most studies, including our previous study10), have evaluated only untreated cases.
In the present study, we undertook to further evaluate the changes of peripheral T lymphocyte subsets in patients with lung cancer following treatment (anticancer chemotherapy and pulmonary resection).
MATERIALS AND METHODS
1. Patients
Forty-nine untreated patients (41 men and 8 women) with primary lung cancer (ages; 38 to 75 years; mean, 57±10 years; 24 squamous, 10 adenocarcinoma, 11 small cell, 4 undifferentiate carcinoma) (Table 1) and 28 normal subjects (23 men 5 women; ages, 45 to 65 years; mean, 55 ± 14 years) were studied.
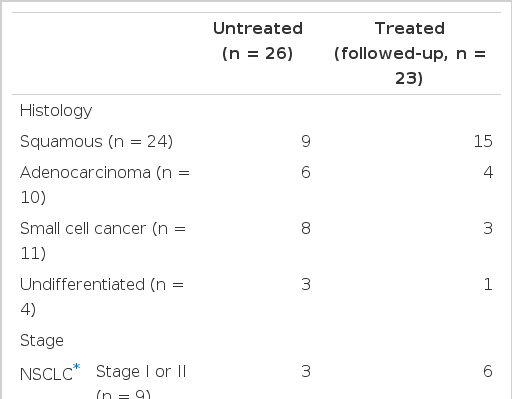
Patients Characteristics According to Histology and Stage (n = 49)
Patients with non-small cell lung cancer (NSCLC) were 38 in number and were staged by the TNM classification. Clinical staging indicated that 9 were stage I or II and 29 were stage III. In the 11 patients with untreated small cell lung cancer(SCLC), 3 were classified as having limited disease(LD) and 8 had extensive disease(ED).
Among 49 patients with untreated lung cancer, 23 had received treatment, of whom 15 had received anticancer chemotherapy alone (3 SCLC, 1 stage I or II, 11 stage III) and 8 had received pulmonary resection alone (stage I or II). Patients who received pulmonary resection or chemotherapy had blood samples taken 2 to 4 weeks after operation and 3 months later after chemotherapy (Cytoxan-Adriamycin-Etoposide or Cisplatin-Etoposide regimen every 3 weeks), respectively.
The assessment of response to anticancer chemotherapy was identical with that described previously17) and postoperative patients were considered to be responders.
2. Evaluation of Peripheral Lymphocytes
The total WBC, lymphocyte counts and percentage of lymphocytes were determined by a Coulter Counter Model S-Plus. The monoclonal antibodies were obtained from Ortho Pharmaceutical Corporation (Raritan, New Jersey, USA). The antibodies used in this study included antibodies OKT4 (helper/inducer) and OKT8 (suppressor/cytotoxic) T-cells.
Peripheral blood mononuclear cells were isolated by Ficoll-Hypaque gradient centrifugation of heparinized blood, were incubated for 30 min. with the monoclonal antibodies and then labelled with a fluorescein-conjugated goat antimouse serum (GAM-FITC, TogoLab, Netherland). Fluorescein cells were counted by means of indirect fluorescent microscope (counted 200 cells), and were expressed as percentage.
3. Statistical Evaluation
Student two-tailed unpaired t test was used to compare mean values of normal controls and of patients, and paired t test was used to compare mean values following treatment (before vs. after treatment).
All results were expressed as mean ± SD.
RESULTS
1) Total WBC counts, lymphocyte counts and percentage of lymphocytes in patients with untreated lung cancer (Table 2)

Total WBC Counts, Lymphocyte Counts and Percent of Lymphocytes in Normal Controls and Patients with Lung Cancer (n = 49)
Total lymphocyte counts and percentage of lymphocytes in patients with lung cancer were decreased significantly compared to normal controls (p<0.02).
Total WBC counts were increased in patients with stage I or II, but total lymphocyte counts in stage III and ED of SCLC, and the percentage of lymphocytes in ED were significantly decreased (p<0.005).
Total WBC counts were increased in squamous cell cancer (p<0.05), and lymphocyte counts were decreased in squamous cell, small cell and undiffrentiated cancer, but there was no significant difference between patients with adenocarcinoma and normal controls. The percentage of lymphocytes was significantly decreased in patients with squamous cell cancer and small cell cancer (esp. ED).
2) Changes of total WBC counts, lymphocyte counts and percentage of lymphocytes after treatment (Table 3)
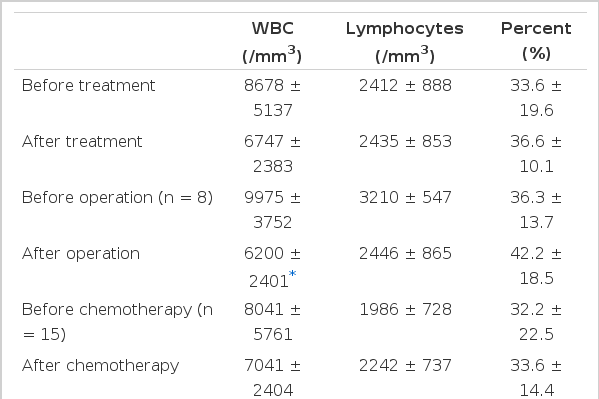
Changes of Total WBC, Lymphocytes and Percent of Lymphocytes with Treatment (n = 23)
Twenty-three patients with lung cancer had received pulmonary resection (n = 8) or anticancer chemotherapy (n = 15). There were no significant differences in the total counts and percentage of lymphocytes, but total WBC counts were significantly decreased after operation compared with before operation (p = 0.02).
3) T-cell subsets in patients with untreated lung cancer (Table 4)

T Cell Subsets in Normal Controls and Patients with Lung Cancer
There was no significant difference between patients with lung cancer and normal controls in OKT4(%). Patients with lung cancer, however, had significantly decreased OKT8(%) (p<0.01).
Patients with undifferentiated carcinoma had significantly decreased OKT4(%) (p<0.05), patients with squamous cell cancer, adenocarcinoma and SCLC had significantly decreased OKT8(%) (p<0.05) and the OKT4/OKT8 ratio was significantly increased in patients with adenocarcinoma. There was no significant difference between any stage of lung cancer and normal controls in OKT4(%), but OKT8(%) was significantly decreased in patients with all stages of NSCLC and ED of SCLC (p<0.02).
There were no significant differences between patients with stage I or II NSCLC and SCLC in OKT4/OKT8 ratio, but patients with stage III NSCLC had a significantly increased OKT4/OKT8 ratio (p<0.02).
4) Changes of T cell subsets following treatment (Table 5)
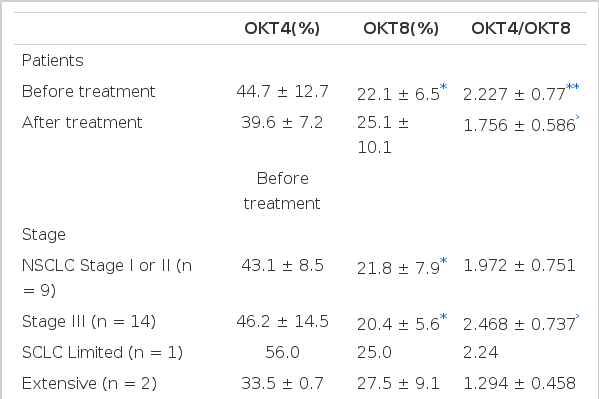
Changes of T Cell Subsets with Treatment (n = 23)
The 23 patients with lung cancer also had significantly increased OKT4/OKT8 ratios (p = 0.02), and this was increased in stage III NSCLC before treatment compared to normal controls. OKT8(%) was also significantly decreased in untreated patients and in all stages of NSCLC compared to normal controls.
There were no significant differences before and after treatment in OKT4(%) and OKT8(%), but OKT8(%) was persistently decreased after treatment compared to normal controls. The OKT4/OKT8 ratio was significantly decreased after treatment compared to before treatment, and was more apparent in patients with stage III NSCLC, which showed no difference between after treatment and normal controls, suggesting improved immunoregulatory functions.
5) Comparison of total WBC counts, lymphocyte counts, percentage of lymphocytes and T cell subsets following treatment according to mode of response (Table 6)
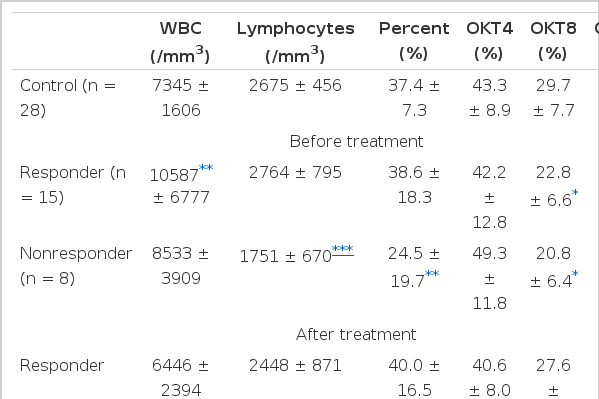
Comparison of Total WBC, Lymphocytes, Percent of Lymphocytes and T Cell Subsets with Treatment According to Mode of Response
Total WBC counts of patients with lung cancer were significantly increased in responders before treatment (p<0.02) compared to normal controls, and total counts of lymphocytes were significantly increased in responders (p<0.03) compared to nonreponders before treatment. Total counts and percentage of lymphocytes before treatment were significantly decreased in nonresponders compared to normal controls and were persistently decreased after treatment (p<0.02).
There were no differences between responders, nonresponders, before and after treatment, or normal controls in OKT4(%). Patients with lung cancer had decreased OKT8(%) in responders and nonresponders before treatment compared to normal controls and had persistently decreased OKT8(%) in nonresponders after treatment.
There were no significant differences between normal controls, before and after treatment, responders or nonresponders in the OKT4/OKT8 ratio.
DISCUSSION
There are many reports that patients with lung cancer often display immune abnormalities,1–10,13,14,18) and these abnormalities in cell mediated immunity have been considered to be significant in the development and progression of lung cancer1,4,9,15,16,20,21,23).
Evaluation of immunocompetence in patients with lung cancer by peripheral total lymphocyte counts,1,4,8–10) percentage of lymohocytes,3) delayed skin hypersensitivity test,6,10,20,21,23) quantitation of peripheral lymphocyte subsets4,5,7,9,10,12) and mitogen stimulation of lymphocytes2,8) has demonstrated both functional and quantitative abnormalities.
However, conflicting data have been reported on the distribution of mononuclear cell populations in patients with lung cancer3–10,11,16,19,22).
In the present study, we evaluated the distribution of peripheral T lymphocyte subsets in patients with untreated lung cancer and changes of T lymphocyte subsets following treatment (pulmonary resection or chemotherapy).
The present investigation revealed that patients with untreated lung cancer had increased total WBC counts in stage I or II NSCLC (esp. squamous cell cancer) compared to normal controls, which were significantly decreased after operation and were also noted in responders. Olkowski et al.3) and Dellon et al.16) found that patients with lung cancer had increased WBC counts, especially in adenocarcinoma, but our study revealed this in squamous cell cancer and we considered that it may be due to distal bronchial obstruction causing inflammation or a pneumonic process.
Patients with untreated lung cancer had significantly decreased percentages and absolute counts of peripheral lymphocytes compared to normal controls, which were more apparent in stage III NSCLC, SCLC (esp. ED) and squamous cell type, but these abnormalities were not changed or improved after treatment.
The nonresponder group had a significant decrease in lymphocyte counts compared to responders before treatment, and had a decrease in percentage and absolute counts of lymphocytes compared to normal controls before and after treatment. We suggest that patients with initial (untreated) lower lymphocyte counts may be possible nonresponders following treatment.
We found that patients with advanced lung cancer had decreased lymphocyte counts, and this finding is in accord with other results1,3,4,7,8,10).
Roberts et al.1) reported that lymphopenia was a feature of patients with metastatic disease of bronchial carcinoma. Krant et al.6) found that circulating lymphocytes were decreased significantly during the months approaching death.
Patients with untreated lung cancer had a significant decrease in OKT8(%) compared to normal controls, and this was decreased in patients with SCLC (esp. ED) and all stages of NSCLC (esp. squamous and adenocarcinoma).
These results are in discord with other results,4,5,7,12) but we confirmed our previous study.10) Ginns et al.23) reported that patients with squamous cell cancer involving lymph nodes (N1 or N2 disease) had a decrease in numbers and percentage of T8 lymphocytes. Because our treated NSCLC cases consisted mainly of squamous cell cancer, decreased OKT8(%) is considered to be consistent with Ginns et al.23) Gross et al.8) found that a decrease in circulating rosette-forming cells was predictive of carcinoma in undiagnosed pulmonary coin lesion. However, Jansen et al.13) and Lichtenstein et al.14) have reported that there were no abnormalities of circulating T cells in patients with lung cancer. Recently, Wesselius et al.4) reported that patients with SCLC and advanced NSCLC had a significant decrease in the number of T4 and T8 cells.
In any case, regardless of whether or not T cell subsets had changed, we consider that these changes would be due to methodologic differences5), compartmentalization into lungs11) or clonal expansion.
Patients with untreated lung cancer had a significant increase in the OKT4/OKT8 ratio compared to normal controls, which was noted in adenocarcinoma and stage II NSCLC, and was considered to be due to the decrease in OKT8(%).
The significance of this finding is open to speculation, but this result is the same as those of other studies.5,10)
After treatment, the decreased OKT8(%) before treatment returned to the normal range in patients with stage I or II NSCLC, but remained persistently decreased in stage III and nonresponders. So, we suggest that patients with advanced lung cancer having low lymphocyte counts before treatment and decreased OKT8(%) after therapy might not be responsive to treatment.
The increased OKT4/OKT8 ratio in stage III NSCLC returned to the normal range, and this finding suggests that immunoabnormalities in patients with lung cancer might be improved following treatment with or without response.
In summary, patients with lung cancer had immunologic abnormalities, such as decreased lymphocyte counts, decreased OKT8(%) and increased OKT4/OKT8 ratios, and these abnormalities might be improved following treatment.
Further data monitoring the quantitative and functional changes (esp. for SCLC) of lymphocytes following treatment (including radiotherapy) are needed to analyse the role of immunologic changes for the progression, recurrence and prognosis of lung cancer.