


INTRODUCTION
Myeloablative conditioning regimens with high-dose chemotherapy, with or without a lethal dose of total body irradiation, have been applied to eradicate underlying disease and suppress the host's immune system to achieve engraftment and disease control in allogeneic hematopoietic stem cell transplantation (HSCT). This type of HSCT causes profound marrow suppression and organ toxicity. Recently, nonmyeloablative stem cell transplantation (NST) has been widely and increasingly used in clinical allogeneic HSCT, based on findings that engraftment can also be succeeded by nonmyeloablative conditioning regimens, which are mainly composed of immune suppression. The term reduced-intensity allogeneic hematopoietic stem cell transplnantation (RIST) is also used for any transplantation that uses a conditioning regimen other than myeloablative. Although a RIST regimen that is of minimal intensity is called NST in a strict sense, the term NST is synonymously used with RIST in the present review. Originally, NST was developed by several researchers about 10 years ago [1-7]. NST is beneficial for older patients (generally over 50-55 years old) and those with comorbidities because nonmyeloablative conditioning regimens are less toxic for the bone marrow as well as the other organs and tissues, resulting in reduced transplant-related mortality (TRM). Other major complication such as graft-versus-host disease (GVHD) usually occur when a conversion occurs from mixed chimerism to complete donor chimerism, which is accompanied by the graft-versus-leukemia (GVL) effect. To obtain complete donor chimerism, donorlymphocyte infusion (DLI) is the usual procedure that supports enhanced engraftment and suppresses the host-versus-graft reaction, and sometimes induces the GVL effect [8-14]. However, similar to allogeneic myeloablative stem cell transplantation, separation of the GVL effect from GVHD is difficult.
Allogeneic immune responses can be induced against other hematological malignancies. An anti-lymphoma or anti-myeloma effect is also observed after allogenic HSCT and is called the graft-versus-lymphoma effect or graft-versus-myeloma effect, respectively. The term GVL effect is used here to include representatives of graft-versus-hematological malignancy effects.
Although NST has been applied to solid tumors such as renal cell carcinoma, breast cancer, and melanoma with a great expectation for a cure, a marked antitumor effect (graft-versus-tumor effect) often accompanies severe GVHD [15,16]. Thus, NST for solid tumors is now being performed only in a limited number of institutions.
Based on the frequent coexistence of a GVL effect with GVHD in NST and conventional myeloablative stem cell transplantation (CST), efficient separation of the GVL effect from GVHD is eagerly anticipated. The separation of the phenomena appears to be realized by progress in transplantation immunology, utilization of minor histocompatibility antigen expression differences between donor and host, tumor-associated antigens for vaccination or cytotoxic T-cell induction, cellular therapies, and new pharmacologic agents. These strategies are beneficial not only for NST but also for CST to enhance the GVL effect without inducing severe GVHD.
Nonmyeloablative stem cell transplantation
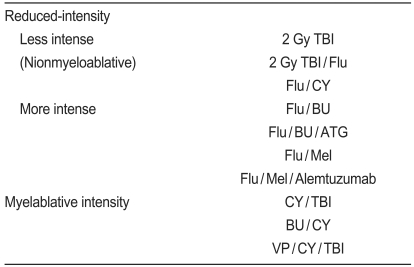
NST was developed by several investigators with various conditioning regimens that are different from conventional myeloablative HSCT (Table 1). The representative CST is as follows: cyclophosphamide (CY) 60 mg/kg├Ś2 days+ total body irradiation (TBI) 2 Gy├Ś12, busulfan (BU) 1 mg/kg├Ś16+CY 50 mg/kg├Ś4 days, and VP-16 10 mg/kg├Ś2 days+CY 60 mg/kg├Ś2 days+TBI 2 Gy├Ś6. In contrast, NST regimens have reduced-intensity compared to those of CST. Each regimen shows somewhat different GVHD incidences and GVL effects. The M.D. Anderson Cancer Center and the UK groups [16-18] use fludarabine (Flu) 30 mg/m2/day├Ś4-5 days+melphalan (Mel) 140 mg/m2/day├Ś1 day┬▒alemtuzumab 20 mg/day├Ś4-5 days. The Hadassah University Hospital group and others [2,19,20] use Flu 30 mg/m2/day├Ś6 days or cladribine 12 mg/m2/day├Ś5 days+BU 4 mg/m2/day├Ś2 days┬▒anti-T-lymphocyte globulin (ATG) 10 mg/kg/day├Ś4 days. The Massachusetts General Hospital group uses Flu 30 mg/m2/day+CY 50 mg/kg/day├Ś4 days+ATG 15 or 30 mg/kg/day├Ś2 days+7 Gy thymic irradiation. The NIH and M.D. Anderson Cancer Center groups [5,15,21,22] use Flu/CY.
The Fred Hutchinson Cancer Research Center group [3,23,24] uses 2 Gy TBI┬▒Flu 30 mg/m2/day├Ś3 days. Among reduced-intensity conditioning regimens, Flu/Mel┬▒alemtuzumab and Flu/BU┬▒ATG are relatively close to the myeloablative conditioning regimens. In contrast, Flu/CY and TBI 2 Gy┬▒Flu are milder conditioning regimens than Flu/BU┬▒ATG and Flu/Mel. Therefore, DLI is often needed to obtain complete donor chimerism in cases with the most reduced-intensity conditioning regimens such as Flu/CY and TBI 2 Gy┬▒Flu. The conditioning regimen intensity correlates with antileukemic activity, regimen-related toxicity, and time to achieve complete donor chimerism. Further descriptions about the differences in each procedure can be found elsewhere. Delineating the incidence of GVHD and GVL effects is more important in NST as well as in CST and it enhances the GVL effect without augmenting GVHD.
NST induces mixed chimerism, followed by a decreased early onset of grades II to IV (mild to severe) acute GVHD. However, late-onset (>100 days after NST) acute GVHD and chronic GVHD occur similarly to those in CST. Initially, the incidence and severity of acute GVHD was thought to be less in NST than in CST because NST results in milder tissue toxicity and does not induce a cytokine storm, which is one of the major inducers of acute GVHD and possibly chronic GVHD [25-28]. Although the incidence and severity of acute GVHD is somewhat delayed in NST compared to CST, it is not much different from those of CST. The only difference is the delayed occurrence of acute GVHD in NST as compared to CST and it partly depends on the delayed establishment of complete donor chimerism and utilization of DLI to inhibit rejection, promote engraftment, and enhance the GVL effect. The DLI dose is not always correlated with GVHD and the GVL effect and unfortunately both phenomena often coexist.
One of the advantages of NST is less toxicity against various organs and tissues; thus, it is applicable to older patients and those with limited organ dysfunction. This is a great advantage for NST because now many patients can receive allogeneic HSCT in a NST fashion. Another advantage is the expected recovery of autologous hematopoiesis, even if engraftment failure occurs; however, this characteristic is correlated with frequent mixed chimerism and relapse of leukemias or other hematological malignancies.
Several studies have shown that the outcomes of older patients who undergo NST during remission are comparable to those of patients who receive CST [29-31], suggesting that the GVL effect associated with NST might be adequate for controlling chemosensitive or slowly progressing disease. Although whether NST is feasible for patients not in remission is controversial [32-35], Maruyama et al. [36] showed that the GVL effect associated with NST is comparable to that associated with CST.
Clinical outcome in hematological malignancies after NST
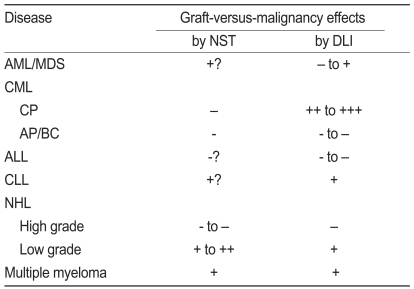
Clinical outcome in various hematological malignancies after NST varies from disease to disease and depends on disease status and its growing capacity (Table 2).
Acute myelogenous leukemia (AML)/myelodysplastic syndrome (MDS)
Regardless of the various conditioning regimens, the occurrence of acute GVHD (Ōēźgrade II), chronic GVHD, 2-year overall survival (OS), and NST relapse rate are about 35%, 40%, 40%, and 50%, respectively, suggesting similar outcomes to those in CST [37,38]. However, NST is superior to chemotherapy in patients older than 50 years with AML and in those in their first complete remission [39]. An additional randomized trial is needed to determine whether NST in younger patients with AML/MDS is also superior to CST.
Chronic myelogenous leukemia (CML)
The Israeli group showed that the 5-year disease-free survival rate for chronic phase CML (CML-CP) is about 85% [40], whereas the European Group for Blood and Marrow Transplantation showed a 5-year OS of about 60% in CML-CP and about a 20% 5-year OS in accelerated phase or blastic crisis CML (CML-AP/BC) [41]. Since new drugs such as imatinib, nilotinib, and dasatinib have been developed and are extensively effective CML-CP agents, the frequency of allogeneic HSCT including NST is decreasing, and allogeneic HSCT is performed only in cases of advanced-phase CML. More intense conditioning regimens rather than minimally reduced conditioning regimens are recommended when NST is chosen for CML [42].
Acute lymphoblastic leukemia (ALL)
Generally, the GVL effect after allogeneic HSCT is hardly generated in ALL, but some GVL effect may occur [43-45]. Furthermore, the GVL effect for ALL might be supported by the result of a retrospective analysis in Japan, which showed that allogeneic HSCT for ALL was superior to autologous HSCT and dissimilar to AML [46]. Another aspect of allogeneic HSCT for ALL is to intensify the conditioning regimen, although NST has more often been performed for various hematological diseases. In fact, an excellent outcome (about a 90% 3-year OS) was observed in allogeneic HSCT using a conditioning regimen with medium-dose VP-16, cyclophosphamide, and total body irradiation for patients with ALL in their first complete remission [47]. NST is not often performed for such patients to justify its efficacy for the GVL effect. In general, because a slight GVL effect may be induced even by the CST setting, NST is likely inadequate for ALL.
Chronic lymphocytic leukemia (CLL)
CLL is an incurable disease with standard chemotherapy. Although autologous HSCT shows little evidence of a beneficial outcome, allogeneic HSCT with myeloablative conditioning regimens have established high and complete response rates but often with high TRM [48]. The presence of a GVL effect in CLL is evident in the induction of complete remission by DLI [48,49]. Therefore, NST has been applied to CLL as well. TRM is reduced by NST, but this benefit is offset by increased relapse rates [50].
Non-Hodgkin's lymphoma (NHL)
Autologous HSCT is usually performed in patients with NHL, and allogeneic HSCT is applied to relapsed, chemoresistant, or poor-prognosis patients. The outcome of NST for high-grade NHL varies widely [22,51,52]. In contrast, low-grade, advanced-phase NHLs, especially follicular lymphoma, are well treated with NST, resulting in about an 80% 3-year OS [53].
Multiple myeloma
Allogenic HSCT with myeloablative conditioning regimens is too toxic to patients with multiple myeloma and results in a higher TRM [54], although a graft-versus-myeloma effect does exist [55,56]. Single or double autologous HSCT is often used for multiple myeloma treatment, but controversial results have been reported [57,58]. NST following autologous HSCT has also been examined and results in an excellent outcome [59,60]. However, controversy still exists concerning the outcome between double autologous HSCT and autologous HSCT followed by NST [61]. Furthermore, better response rates are obtained using various new drugs such as tahidomide, lenalidomide, and bortezomib in combination with dexamethasone, prednisolone, and/or melphalan, and when using those as maintenance therapeutic drugs after single autologous HSCT [62-64]. So, the efficacy of NST for multiple myeloma has not yet been confirmed.
DLI and graft-versus-hematological malignancy effects
DLI is often required to achieve complete donor chimerism in minimally reduced-intensity conditioning regimens. However, it is not so frequently required to achieve complete donor chimerism after moderately reduced-intensity conditioning regimens, which are similar to myeloablative conditioning regimens; therefore, it is currently used only for relapse or after an increase in host cells during a period of mixed chimerism. Table 2 summarizes the anti-hematological malignancy effects by DLI in various hematological diseases.
Initially, DLI was reported to be markedly effective against CML relapse after allogeneic HSCT. About 80% of patients treated with DLI for relapsed CML-CP will achieve a complete cytogenetic and molecular response [14,65]. In contrast, only 12-28% of patients with accelerated phase or blast crisis relapse respond to DLI. Advanced-phase relapse rates after DLI are high [66,67]. Although DLI results in an excellent GVL effect against relapsed CML, its effect is disappointing inrelapsed AML, exhibiting about 20-30% complete remission [14,65]. Furthermore, DLI is less effective for managing posttransplant MDS. The GVL effect of DLI is not remarkable in cases of ALL, showing only about a 10% complete remission [65]. The response rate for DLI in patients with multiple myeloma is about 30%, but a sustained remission occurs in 0-18% of patients [55,68-70]. In addition to the limited response rate, DLI toxicity is significant for myeloma, with more than half of patients experiencing acute and chronic GVHD. Therefore, a graft-versus-myeloma effect has been implicated in other settings such as RIST or the prophylactic use of DLI following T-cell-depleted HSCT. [71,72]. Furthermore, new drugs such as bortezomib and thalidomide are often used for myeloma in combination with other drugs, so the advantage of allogeneic HSCT for the treatment of multiple myeloma is being reconsidered. Although Hodgkin's lymphoma (HL) and NHL are susceptible to the DLI graft-versus-lymphoma effect to some extent [52,73-75], the GVL effect appears to be readily generated in the NST setting for HL and low-grade NHL [53,76]. Acute GVHD develops in 19-33% of DLI after NST, and chronic GVHD occurs in 33-34%. No statistically significant relationship exists between GVHD and DLI dose in some occasion [77,78].
Chimerism and DLI
DLI is performed to avoid graft rejection or malignancy relapse and is marginally effective for controlling such episodes, although not always. A chimerism analysis, which shows the proportion of donor-derived and host-derived cells, is important to determine the appropriate timing for DLI. Several methods can be used to analyze chimerism. Among them, using microsatellite DNA as the RT-PCR probe is useful in terms of accuracy and quantity [79]. Although donor T-cell chimerism is believed to be a good indicator for estimating engraftment and rejection, donor NK-cell chimerism at the early phase after transplantation is also a valuable indicator [79,80]. BecauseNK cells recover faster than T cells, donor NK-cell chimerism predicts subsequent donor T-cell chimerism and engraftment. Murine models suggest the importance of host NK cells for rejection of allogeneic hematopoietic stem cells [81-83]. In fact, more frequent rejection occurs when donor CD56+ NK-cell chimerism is less than 50% on day 14, resulting in an unfavorable outcome [79]. Grade II to IV acute GVHD develops in patients with more than 50% donor-type chimerism in CD3+ T cells on day 14. Furthermore, more than 50% of donor-type chimerism in CD56+ NK cells on day 14 and more than 75% donor-type chimerism in CD3+ T cells, CD56+ NK cells, and CD14/15+ myeloid cells on day 28 are associated with a lower relapse rate. Better 1-year overall survival is shown in patients with more than 50% donor-type chimerism in CD56+ NK cells on day 14 and more than 90% donor-type chimerism in CD14/15+ myeloid cells and CD56+ NK cells on day 28.
Regarding the GVL effect, Baron et al. [84] reported that extensive chronic GVHD, but not acute GVHD, is associated with a decreased risk of relapse or progression and an increased probability of progression-free survival. Although achievement of complete donor chimerism was associated with a decreased risk for relapse or progression, grade II to IV acute GVHD had no significant impact on the risk of relapse or progression but was associated with an increased risk for non-relapse mortality and decreased probability of progression-free survival. The reason why acute GVHD was not associated with an increased probability of achieving complete remission in their study appeared to be that corticosteroids and other immunosuppressive agents used to treat acute GVHD lowered the GVL effect.
In any case, a chimersim analysis on various cell lineages, such as CD3+ T cells, CD56+ NK cells, and CD14/15+ myeloid cells, is important to estimate the appropriate timing of DLI and to evaluate the occurrence of rejection, relapse, and GVHD in NST.
Role of antigen peesenting cells (APC) in the induction of GVHD and graft-versus-hematological malignancy effects
The presence of host-derived APCs during the first month after NST may be responsible for efficient donor T-cell immunization against host hematopoietic cells. Strong antileukemic responses are seen in some patients without clinical GVHD, suggesting that those responses were directed against antigens preferentially expressed on hematopoietic cells, although this situation cannot exclude the existence of a subclinical level of graft-versus-host reaction (GVHR). In general, achievement of complete donor T-cell chimerism is associated with a reduced risk of relapse or progression, indicating that alloreactivity against both normal host hematopoiesis (GVHR or GVHD) and leukemic cells (GVL effect) were effectively induced.
However, complete donor chimerism increases non-relapse mortality. This observation can cause the apparent strong association between high levels of donor T-cell chimerism early after NST and the increased risk of more severe GVHD. Therefore, a transient mixed chimerism after NST appears to be requisite to induce the GVL effect, and possibly GVHR/GVHD as well, through donor T-cell immunization by host APCs. In fact, the absence of host APCs by day 100 after NST leads to reduced acute GVHD [85], whereas the GVL effect can be induced by crosspresentation in which donor T cells are primed with host leukemia antigens presented by donor APCs [86]. Host APCs, however, have recently been suggested as being necessary to induce both the GVHD and GVL effect; moreover, APCs were also found to be necessary to induce both the GVHD and GVL effect, showing the absence of a clear association between donor/host APCs and the GVHD/GVL effect. Although Matte et al. [87] reported that GVHD is intensified by donor APCs cross-priming alloreactive CD8+ T cells, and that donor APCs are not required for the CD8-mediated GVL effect, Reddy et al. [88] showed that APCs and alloantigen tumor expression are crucial for the GVL effect, and that host APCs predominate in the GVL effect with the contribution of donor APCs to decrease tumor burden. Furthermore, donor or host APCs are associated with CD4-mediated chronic skin GVHD via CD80/CD86 dependent costimulation, and both donor and host APCs elicit maximal chronic GVHD, whereas donor APCs play a dominant role in CD4-mediated intestinal chronic GVHD via CD40 and CD80/CD86-dependent costimulation [89]. Because host APCs are required to initiate CD8-mediated acute GVHD [90,91], differences in APC requirements exist between CD8-mediated acute GVHD and CD4-mediated chronic GVHD, with target tissue-specific differences as well.
Separation of graft-versus-hematological malignancy effects from GVHD
The separation of the GVL effect from GVHD is one of the major issues in allogeneic HSCT. Various trials have been conducted to examine such conditions in murine models. For example, utilization of a cytokine balance toward Th1/Tc1 may preferentially lead to the GVL effect. A special T-cell subset expressing CD62L- CD4+ effector memory T cells appears to play an important role for exerting the GVL effect without augmenting GVHD. Utilization of alloreactive NK cells can deplete host APCs, resulting in reduced GVHD with a preserving GVL effect. Blockade of costimulatory molecules such as CTLA4-Ig, anti-OX40L antibody, and anti-ICOS antibody may inhibit GVHD and preserve the GVL effect [92-98]. Chemokine and chemokine receptor modulation by the relevant antibody or antagonist may also inhibit GVHD, but not the GVL effect [99-108]. Novel pharmacologic agents such as the proteasome inhibitor bortezomib plus allogeneic T-cell infusion induce the GVL effect without enhancing GVHD [109]. Furthermore, the histone deacetylase inhibitor suberoylanilide hydroxamic acid induces the GVL effect, but not GVHD [110].
In humans, alloreactive NK cells can inhibit GVHD and preserve the GVL effect, so in vivo expansion after allogeneic HSCT and transfer of in vitro-generated alloreactive NK cells appear to inhibit GVHD, but not GVL or the graft-versus-tumor effect [91,111-113]. Rapamaycin appears to induce the GVL effect, inhibiting GVHD in humans [114,115]. Recently, CCL8 has been shown to be a molecular candidate for the diagnosis of acute GVHD in both mice and humans [116,117], and a four protein fingerprint of interleukin-2 receptor-╬▒, tumor necrosis factor receptor-1, interleukin-8, and hepatocyte growth factor in plasma have been identified as biomarkers for predicting severe acute GVHD [118]. Therefore, determining whether blocking of these molecules inhibits GVHD and preserves the GVL effect would be of interest.
Differences in minor histocompatibility antigen expression between donor and host can be utilized to separate the GVL effect from GVHD, although a limitation exists in exploiting such disparities in terms of difficulty in HLA-matched donor selection and HLA-restricted immune response of anti-minor histocompatibility antigens [119-121]. HA-2 is preferentially expressed on hematopoietic tissue rather than nonhematopoietic tissue; therefore, anti-host HA-2-specific T cells induce the GVL effect without augmenting GVHD. In contrast, HA-1 is expressed on both hematopoietic and non-hematopoietic tissues, and HA-3 is preferentially expressed on nonhematopoietic tissues, suggesting that these minor histocompatibility antigens are not suitable to induce only the GVL effect. The Y chromosome encodes male-specific minor histocompatibility (HY) antigens such as UTY, SMCY, and DBY; therefore, anti-HY-specific T cells can be induced after female to male allogeneic HSCT [122-124]. Because only UTY is modestly expressed on host epithelial cells, anti-UTY-specific T cells may lead to the GVL effect without augmenting GVHD. In contrast, SMCY and DBY are highly expressed on epithelial cells, thus causing anti-SMCY- and DBY-specific T cells that appear to induce both GVHD and the GVL effect. Furthermore, DDX3Y, which is expressed on leukemic stem cells, appears to be a suitable target for the GVL effect, but not for GVHD, because DDX3Y expression is detected in all myeloid and lymphoid leukemic cells that carry an intact Y chromosome [125].
Other candidate antigens that exert only the GVL effect, but not GVHD, are as follows: proteinase 3, which is aberrantly expressed or overexpressed in AML and CML [126-128]; WT-1 in AML, CML, and multiple myeloma [129-132]; survivin for AML, CML, CLL, and lymphoma [133-136]; idiotype for multiple myeloma [137]; and BCR-ABL [138] for CML. In vitro-generated cytotoxic T cells against various minor histocompatibility antigens can be used for adoptive transfer, and peptide vaccine trials for BCR-ABL, PR1 derived from PR3, and WT1 are being examined. The efficacy of the BCR-ABL vaccine is limited in patients with low levels of residual and stable disease. In contrast, the PR1 and WT1 vaccines are more beneficial, resulting in better clinical responses [139]. However, vaccination therapy with only these peptides is not enough to obtain a sufficient clinical outcome. Recently, unique HLA-mismatch combinations between donor and host HLA-C expression have been correlated with the induction of an efficient GVL effect without augmenting GVHD by a retrospective analysis using data from the Japan Marrow Donor Program [140,141]. This type of approach is one of the candidates for separating the GVL effect from GVHD, although great genetic differences exist among nations regarding GVHD and HLA disparities.
CONCLUSION
The efficacy and limitations of NST are becoming clearer because this procedure alone cannot sufficiently induce the graft-versus-hematological malignancy effect except for certain diseases, even in combination with DLI. Therefore, future progress in transplantation immunology is needed, so that we are able to efficiently separate graft-versus-hematological malignancy from GVHD. Furthermore, NST should be combined with various strategies such as the utilization of minor histocompatibility antigen expression differences, vaccination, or induction of cytotoxic T cells using tumor-associated antigens and other cellular therapies to enhance the graft-versus-hematological malignancy effect without augmenting GVHD.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





