


INTRODUCTION
Volatile organic compounds (VOC) are comprised of 3 major components: aliphatic hydrocarbons (chloroform, carbon tetrachloride), petroleum products (gasoline, mineral oil) and aromatic hydrocarbons (benzene, toluene, xylene)1).
Among the VOCs, aromatic hydrocarbons are widely used as industrial solvents and dry cleaning agents in the rubber and shoe industries and for printing and paper-coating2).
The chemicals in this category are readily absorbed through the lungs, skin and gastrointestinal tract, which can cause headaches, dizziness and liver or kidney toxicity. Furthermore, there is concern about their potential carcinogenicity and adverse reproductive effects at low levels of exposure3).
Despite the wide distribution of ambient air pollutant VOC sources, the indoor VOC concentrations may be the dominant contributor to personal exposure given that most people spend a large portion of their time indoors4).
The numerous indoor sources for VOCs in a typical residence or building, as well as the contribution from airborne outdoor inflow, result in a wide range of indoor VOCs. Measurement of VOCs in the indoor environment has received substantial research attention during the recent years because the indoor VOC levels may pose potential negative health effects to the occupants5-10).
The concentrations of indoor VOCs can be affected by outdoor atmospheric conditions, the indoor sources that generate VOCs, the indoor volume, the activities of people, removal by reactions, the ventilation rates and seasonal factors. Furthermore, the concentrations of indoor VOCs can vary due to chemical reactions in the presence of ozone, temperature changes and different levels of humidity.
There are many kinds of rooms in a general hospital such as general wards, outpatient clinics, intensive care rooms and hemodialysis (HD) rooms. Among these, the HD rooms have aroused special interest.
In general, HD rooms share many common environmental characteristics. First, the HD machines are compactly arranged in a given space for convenience (a short distance is required between the beds and the nurse station). Second, HD machines continuously run about 10-15 hours a day according to the number of HD sessions. Third, the dialyzer and associated tubing systems are made of polyflux S, soft and rigid polyvinylchloride, acrylonitrile butadiene styrene, high density polyethylene, polyester and rubber (Gambro Dialysatoren, Hechingen, Germany), and all this is opened to the room air at the end of each HD session. Fourth, the HD room temperature is kept relatively higher than most other rooms in the hospital because the patients on HD usually have cold intolerance11, 12). For this reason, the ventilation of the HD room is done not by opening windows, but by a closed air condition control system.
Therefore, the air pollution in an HD room may greatly differ from various other clinical settings13).
Those patients with end-stage renal disease and who are on HD usually stay in a HD room 15-18 hours a week through their lives14). The indoor air pollutants of a HD room may affect the health of not only the patients on HD, but also the medical teams working in the HD room.
This study is designed to compare the VOC concentrations in a HD room with those VOC concentrations of other various clinical settings in a hospital.
MATERIAL AND METHODS
Two target VOCs (benzene and toluene) were chosen for analysis because of their potential to cause adverse health effects and for making comparison with the prior research. The VOCs were measured using a passive sampler, that is, a 3M organic vapor monitor #3500 (www.3M.com/occsafety).
A total of forty passive air samplers were placed in a HD room and in a nearby nursing room of a general ward for 72 hours from May 29 to May 31, 2006 in Soonchunhyang Cheonan Hospital. Five air samplers were hung on the ceilings and placed on the top of tables in both the HD room and the nursing stations that were nearby, but outside the HD room. Five samples were taken from the breathing zone (using a badge on the suit collar) of the nurses in both the HD room and in the general ward (the same ward where the ceiling and table air samplers were placed) during the same study period.
In the general ward nursing station, the duty nurse passed the air samplers to the next duty nurse so that the samplers were worn without interruption for 72 hours.
In the HD room, because the nurse's duties were completed by 10 PM, the air samplers were placed on top of a table in the nurses' station until the next morning at 7 AM when the next nurse began their duty for the first session of HD. When nurses left their station for various reasons (i.e., meal time, going to the toilet, etc.), they detached their sampler badge and placed it on their station table.
In the same way, ten samplers were placed on the edge of the bed in the HD rooms to represent the breathing zone for the patients who underwent HD (within 30 cm from the nose of the patient, who was in the supine position). During the 72 hours period, the beds were occupied by the HD patient for 45-48 hours.
During the sampling period, the temperature was recorded to be between 26~28.5℃ in the HD room and between 25.5~28.0℃ in the ward station. The humidity was recorded as between 31~35% in the HD room and between 29~30% at the ward station.
The main building of the hospital was built in 1981 (25yrs old) and the HD room was remodeled 12 months before the start of the study. In order to get into the HD room from the outside, a person had to pass through 4 separate doors. There were two doors between the outer door and the ward nurse station in the general ward. The ward nurse's station was located at the entrance of the corridor and the air flow was practically uninhibited between the outside and the nurse station by the doors because so many people passed through the doors. There were 18 rooms for the patients on both sides of a corridor and there was another door between the room and the corridor.
The total space of the renal unit was 306 m2, of which 198 m2 comprised the HD room. Twenty-eight HD machines (23 GAMBRO, 5 FMC) with the same number of beds were evenly installed in the HD room. One side of the HD room faced toward the outside air, but the windows were usually closed during the HD section. The average time the windows were open for ventilation was less than 30 minutes during the 72 hour period. One hundred one patients with end stage renal disease (ESRD) regularly underwent hemodialysis for 15~18 hours a week. Their demographic characteristics are summarized in Table 1.
All the air samplers were analyzed at the same laboratory Our method for sample analysis has been described previously15). In brief, the passive samplers were desorbed by adding 1.5 mL of carbon disulfide and then the samplers were agitated; we allowed the badges to be desorbed for 30~45 minutes. The desorbate was then sealed into auto-sampler vials and it was analyzed by GC/MS. The GC oven was programmed to maintain the temperature at 60℃ for 2.5 minutes, followed by heating at 100℃ for 30min, and finally heating at 50℃/min to 200℃ when the temperature was held for 1min.
The desorption efficiencies were taken from the 3M literature that came with the sampler. The samplers were shipped to the laboratory by field researchers. Half the limit of detection (LOD) for each compound was used for the analyses of the samples in which a certain compound was not detected.
Statistics: All the data was expressed as means with standard deviations. Statistical analysis was performed using the ANOVA test to test the differences between 3 or 4 groups, and t-tests was used to compare the data between two groups. p values <0.05 were considered to be statistically significant.
RESULTS
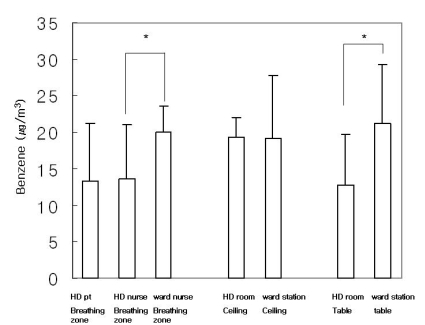
There was no significant difference in the benzene concentrations in the HD room between the ESRD patient's breathing zone (13.3±7.9 g/m3), the nurse breathing zone (13.7±7.4 g/m3), the ceiling (19.4±2.6 g/m3), and the table samples (12.8±6.9 g/m3) (p=0.617). The benzene concentration in the general ward's nurse station was 20.1±3.4 g/m3 for the nurse breathing zone, it was 19.2±8.6 g/m3 for the ceiling and 21.2±8.0 g/m3 for the table (p=0.204). The benzene concentration of the nurse breathing zone was significantly higher in the general ward as compared to the HD room (p=0.006) (Figure 1). Also, the benzene concentration on the table was higher in the general ward station as compared to that of the HD room (p=0.028) (Figure 1), but there was no significant difference in the ceiling benzene concentration, as compared to the general ward station and HD room.
The toluene concentrations in the HD room was 16.1±8.9 g/m3 for the ESRD patient breathing zone, it was 23.3±3.0 g/m3 for the nurse breathing zone, 17.1±1.4 g/m3 for the ceiling and 17.8±6.9 g/m3 on the table (p<0.05, ANOVA test) (Figure 1). However, the toluene concentration was significantly higher in the nurse breathing zone (35.0±4.7 g/m3) as compared to that of both the ward's ceiling (14.9±4.0 g/m3) and table (15.9±2.4 g/m3) (p=0.001) (Figure 2).
The toluene concentration of the nurse breathing zone was also significantly higher in the general ward's nurse stations as compared to that in the HD room (p=0.01, Figure 3).
DISCUSSION
Benzene is used widely not only as a solvent, but also for synthesizing chemicals. Its major acute toxicity primarily affects the central nervous system, while chronic exposure is known to cause leukemia or aplastic anemia with exposure to as little as 1 ppm in the atmosphere16). Toluene has replaced benzene as a solvent because it does not produce leukemia or aplastic anemia, although it is known to cause central nervous system depression17).
Contrary to our expectation, the toluene concentration (p=0.01), and the benzene concentration (p=0.006) of the nurse breathing zone were significantly higher at the general ward nurse station than in the HD room. Also, the benzene concentration in the table sample was higher at the general ward station than that of the HD room (p=0.028).
These findings imply that indoor air pollutant VOCs in the HD room are not worse than that of other rooms in the same building, and this despite the many potential risk factors in a HD room (the compact arrangement, the long running time of the HD machines, exposure of the dialyzers and the associated tubing systems, which are made of polyflux S, polyvinylchloride, acrylonitrile butadiene styrene, high density polyethylene, polyester and rubber, to the room air and the relative high temperature and humidity in the HD room).
Basically, the indoor VOC concentrations are multifactorial and they are the result of outdoor airborne inflow, a wide variety of potential indoor sources of VOCs and the ventilation and/or purification system that's used for the indoor air of the building. In the same way, the VOCs concentration in the HD room would be under the influence of the outdoor concentration, the indoor sources of VOCs and the ventilation system of the HD room.
It is well known that the outdoor VOC concentrations in a metropolitan zone of a large city are high due to the high traffic volume, industrialization and crowded habitation18). The purpose of our study was to see whether the VOC concentrations were higher in the HD room as compared to other similar rooms in the same hospital building (the outdoor VOC concentrations were not focused on in the current study). In our previous study, the ambient out door air concentrations of benzene and toluene were 21.6±11.8 g/m3 and 18.1±14.1 g/m3, and respectively, these were relatively lower levels in HD rooms than those of the capital city Seoul (benzene: 39.8±77.1 g/m3, toluene: 147.8±179.4 g/m3)15).
The sampling device in the current study was designed to measure the average concentrations of certain VOCs over a measured time interval. It can be used for monitoring either personal or an area. For monitoring a person, it is normally worn near the breathing zone of an individual who is exposed to potentially hazardous environments. When it is used as an area monitor, it may be placed on walls, corners, table tops or other regions where the air movement in the room may be limited. In our study, we hung the sampling devices on the ceiling and we placed them on table tops. There was no significant difference noted between these two sampled areas.
However, both the benzene and toluene concentrations were higher in the nurse breathing zone samples. We believe that this was due to the nurses traveling into several rooms along the corridor where the VOC concentrations may have been higher.
VOCs may be present at concentrations that are not considered actually harmful to human health. However, because the lack of a precise cut-off value that's known to be safe, carefully monitoring VOC concentrations is required, and especially in a room inhabited by patients with multiple comorbidities, such as those patients on HD.
In conclusion, both the benzene and toluene concentrations in the HD room were not significantly higher as compared to other rooms in the same building. This finding suggests that both the benzene and toluene concentrations in a HD room are more dependent on the outdoor atmospheric conditions and they are less affected by indoor sources. Ventilating a HD room would be better performed by a centralized air conditioning system rather than by opening windows, and especially when the hospital is located in an outdoor environment with known high levels of VOCs.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





