


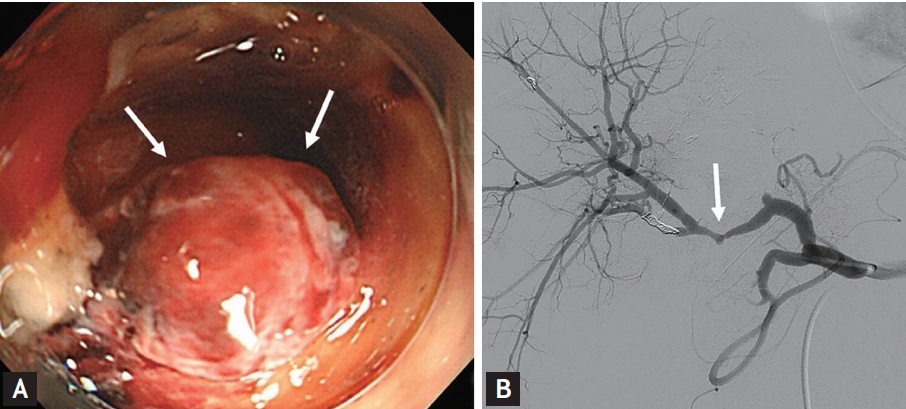
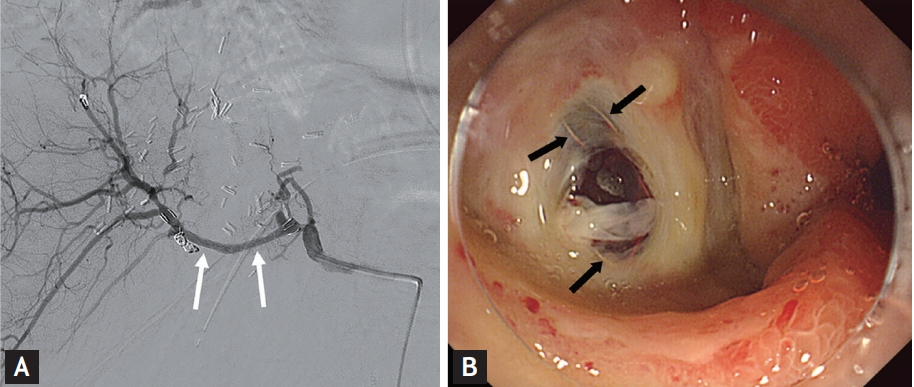
A 76-year-old man was admitted because of hematemesis, anemia, and hypovolemic shock. He had a history of left hepatectomy, bile duct resection, and chemoradiotherapy for cholangiocarcinoma. Emergent gastroscopy revealed active duodenal ulcer with pulsating pseudoaneurysm in the duodenal bulb (Fig. 1A). Subsequent celiac angiography revealed focal aneurysmal dilatation with a stenotic portion of the proximal right hepatic artery corresponding to the pulsating pseudoaneurysm observed on endoscopy (Fig. 1B). Transarterial embolization (TAE) was performed to treat a pseudoaneurysm. However, massive rebleeding occurred 1 day after the TAE. With the help of emergent angiography, transarterial stent-graft insertion was performed in the pseudoaneurysm where the TAE had previously been performed (Fig. 2A). After the procedure and medication for active duodenal ulcer, follow-up endoscopy was performed. The treated pseudoaneurysm with stent-graft insertion was directly visualized along with the healing duodenal ulcer on endoscopy (Fig. 2B). The patientŌĆÖs general condition had improved at discharge and the bleeding did not recur.
This case raises two aspects of clinical interest. First, there are no previous reports of direct endoscopic viewing of an inserted vascular stent after a pseudoaneurysm of a duodenal ulcer was treated with transarterial stent-graft insertion. Second, no clear guideline has been issued regarding the optional treatment of intractable gastrointestinal ulcer bleeding. We hope our experience may support the consideration of rescue treatment for similar patients. In our patient, transarterial stent graft was a good treatment option when the endoscopic and TAE treatments failed. Written informed consent was obtained.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





