


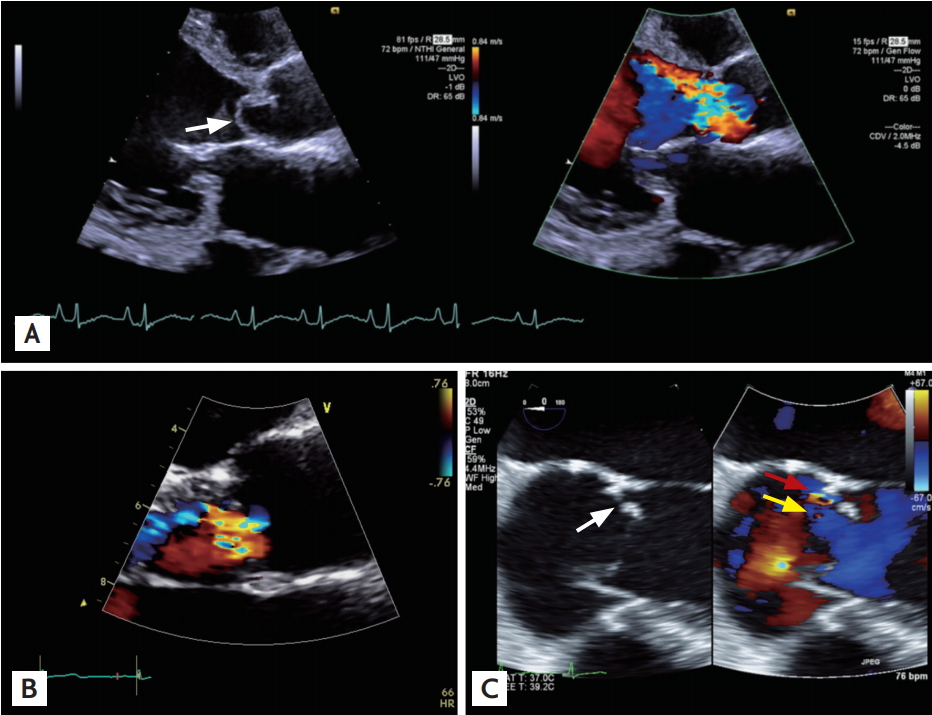
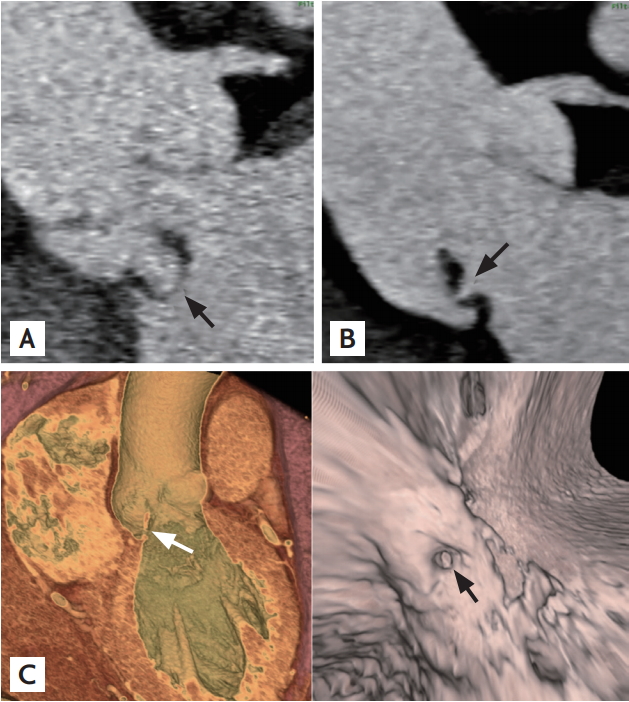
A 64-year-old man with moderate to severe aortic regurgitation without subjective symptoms who was followed for 7 months presented to the outpatient clinic with dyspnea. He had no history of fever or chills. C-reactive protein was elevated. Transthoracic echocardiography (TTE) revealed severe eccentric aortic regurgitation due to a prolapsed aortic valve (left coronary cusp and non-coronary cusp) and malcoaptation (Fig. 1A). These findings were worse than demonstrated on TTE 8 months prior (Fig. 1B). For the evaluation of coronary artery disease before elective aortic valve replacement, cardiac computed tomography (CT) was performed and demonstrated non-coronary cusp prolapse consistent with TTE as well as additional perforation (Fig. 2). Then, transesophageal echocardiography (TEE) confirmed the presence of a 2-mm-sized perforation in the non-coronary cusp (Fig. 1C). In the surgical field, there was a deformity in the non-coronary cusp and right coronary cusp. After diagnosis with culture-negative endocarditis, the patient was treated with 4 weeks of ampicillin-sulbactam and 2 weeks of gentamicin. The patient recovered and was discharged uneventfully. We received informed consent from the
patient. In this case, aortic valve perforation, which did not appear on TTE, was demonstrated on a three-dimensional reconstruction of electrocardiography-gated cardiac CT. The perforation was confirmed on TEE. Anatomical information regarding the coronary artery and great vessels obtained via CT could be useful for surgical planning.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |