


INTRODUCTION
One concern associated with tumor necrosis factor (TNF) inhibitors is the increased risk of reactivation of latent Mycobacterium tuberculosis in patients with rheumatoid arthritis (RA). Therefore, screening and treatment for latent tuberculosis infection (LTBI) is recommended before starting TNF inhibitors. There are several treatment regimens available for the treatment of LTBI. One option includes isoniazid (INH), with the 9-month regimen preferred over the 6-month regimen due to higher efficacy. In addition, the 12-dose once-weekly regimen of INH and rifapetine is recommended as an equally effective option to the standard INH 9-month daily regimen, while a 4-month regimen of rifampin can be considered for patients who cannot tolerate INH [1-3].
Some physicians have concerns about treating patients for LTBI. These concerns are generally related to the length of treatment and the potential side effects of each medication. Asymptomatic elevation of serum liver enzyme concentrations occurs in 10% to 20% of patients taking INH, though these levels usually return to normal. Clinical hepatitis occurs in about 0.1% of patients taking INH [4], which could increase if INH is combined with other hepatotoxic agents such as methotrexate (MTX) and leflunomide.
The potential hepatotoxicity of INH is of concern in RA patients treated with not only conventional disease-modifying anti-rheumatic diseases (DMARDs) [5-7] but also TNF inhibitors [8,9]. A previous report showed that half of RA patients treated with INH experienced liver function test (LFT) abnormalities and suggested that the incidence of hepatotoxicity due to INH in RA patients treated with MTX, sulfasalazine and TNF inhibitors was high [8]. Potential hepatotoxicity of INH can lead to discontinuation of concomitant MTX and it may result in reducing the effectiveness of TNF inhibitors. In addition, patients who cannot treat the LTBI may stop their TNF inhibitor. However, previous studies were performed in a small number of RA patients and the impact of INH treatment on the persistence of TNF inhibitors has not been studied.
We sought to identify the risk of INH treatment for LTBI on LFT abnormality and to evaluate the impact of INH treatment on the persistence of TNF inhibitors in RA patients.
METHODS
Data source
The retrospective registry of Korean RA patients who used biologic DMARDs (REtrospective study for Safety and Effectiveness of Anti-RA treatment with biologiCs [RESEARCh]) was used to evaluate the risk of LFT abnormalities due to INH treatment for LTBI and their impact on the persistence of TNF inhibitors [10]. We identified patients who had ever taken biologic DMARDs between December 2000 and June 2011 from medical records of one university hospital, and enrolled these patients in the RESEARCh database. Comprehensive chart reviews for all patients were undertaken by well-trained health professionals. Demographics, disease activity, comorbidities, treatments, and laboratory data at the first dose of biologic DMARDs were recorded. Treatments, disease activity, and serious adverse events during treatment with biologic DMARDs were also collected.
The RESEARCh study was approved by the Institutional Review Board (HYUH IRB 2010-R-71), and informed consent was waived because the data was de-identified and collected retrospectively.
Participants
Among 442 RA patients who used TNF inhibitors, we included 312 patients who had sufficient data available on disease activity and liver enzyme concentrations. Patients who had hepatitis B or C virus (n = 11), insufficient data on LFTs or LTBI treatment (n = 39), or lack of initial disease activity data (n = 80) were excluded.
Patients were divided into two groups based on the occurrence of LFT abnormality during the use of TNF inhibitors. The mean observational period was 27.8 ┬▒ 23.1 months in patients with LFT abnormality and 23.1 ┬▒ 22.6 months in patients without LFT abnormality. We defined LFT abnormality as any elevation of alanine aminotransaminase (ALT)/aspartate aminotransaminase (AST) levels during TNF inhibitor treatment. LFT is usually monitored every 3 to 6 months after starting TNF inhibitors. To evaluate the early safety of TNF inhibitor, the data collection at 3 months of TNF inhibitor use was also performed. Patient-reported LFT abnormality was also included in the LFT abnormality group.
Statistical analysis
To compare the baseline characteristics between groups who experienced LFT abnormality and those who did not, the chi-square test was used to compare categorical variables and the Student t test was used for continuous variables. A multivariable logistic regression model was used to identify the impact of INH treatment for LTBI on the occurrence of LFT abnormality in RA patients with TNF inhibitor treatment.
A Kaplan-Meier curve and a log-rank test were used to compare the persistence rate of TNF inhibitors between patients who did and did not receive INH treatment. Cox proportional hazards analysis was used to evaluate the impact of INH treatment on the persistence of TNF inhibitors.
These statistical analyses were conducted using SAS 9.2 (SAS Institute, Cary, NC, USA). All p values were twotailed and p < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics of TNF inhibitor users who experienced LFT abnormality
Among 312 patients (595.0 person-year), 39 patients (12.5%) experienced LFT abnormality during TNF inhibitor use, while the other 273 patients did not. The duration of TNF inhibitor use was similar between the two groups, at 27.8 ┬▒ 23.1 months in patients with LFT abnormality and 23.1 ┬▒ 22.6 months in patients without LFT abnormality. In patients with LFT abnormality, the proportion of males was higher (33.3% vs. 12.1%, p < 0.01), while the mean age (49.4 ┬▒ 11.6 vs. 50.4 ┬▒ 13.5, p = 0.66), disease duration (8.2 ┬▒ 6.2 years vs. 9.0 ┬▒ 7.1 years, p = 0.55), and disease activity score-28 joints (DAS28) when starting TNF inhibitors (6.2 ┬▒ 1.1 vs. 5.9 ┬▒ 0.9, p = 0.14) were comparable between the two groups. The value of LFT was 24.5 ┬▒ 13.6 (AST) and 26.8 ┬▒ 23.3 (ALT) in patients with LFT abnormality, and 18.5 ┬▒ 9.1 (AST) and 18.1 ┬▒ 15.6 (ALT) in patients without LFT abnormality.
INH was more commonly used in patients with a history of LFT abnormality (51.3% vs. 27.8%, p < 0.01). However, MTX was more commonly used in patients without LFT abnormality (69.2% vs. 84.3%, p = 0.04), while the prevalence of NSAIDs, glucocorticoids, and the type of TNF inhibitors did not differ between the two groups (Table 1).
Risk of LFT abnormality in RA patients taking INH treatment for LTBI
Unadjusted analysis revealed a significant association between INH treatment and the occurrence of LFT abnormality (odds ratio [OR], 2.73; 95% confidence interval [CI], 1.38 to 5.39). LFT abnormality before starting TNF inhibitors (OR, 2.92; 95% CI, 1.07 to 7.99) was also associated with LFT abnormality during TNF inhibitor use. INH treatment (OR, 3.01; 95% CI, 1.39 to 6.48) was significantly associated with LFT abnormality on multivariable regression analysis after adjusting for other confounding factors. High disease activity when starting TNF inhibitors (OR, 1.55; 95% CI, 1.02 to 2.37) and overweight defined by body mass index Ōēź 23.0 (OR, 1.53; 95% CI, 1.02 to 2.37) were other risk factors for the occurrence of LFT abnormality, while the concomitant use of MTX was protective (OR, 0.31; 95% CI, 0.13 to 0.77) (Table 2). Although INH treatment carried a significant risk of LFT abnormality, the severity of these abnormalities was relatively low. In patients with LFT abnormality identified via laboratory tests, elevation of ASL/ALT was mild (< 3 ├Ś upper limit of normal [ULN]) in all patients.
Impact of INH treatment for LTBI on the persistence of TNF inhibitors
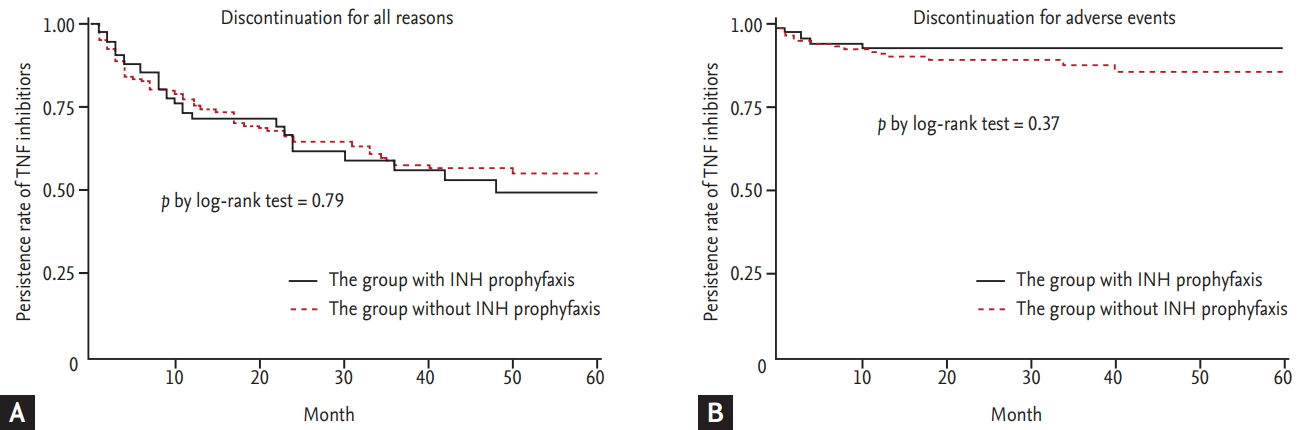
When we divided the patients according to INH treatment, 20 of 96 patients (20.8%) with INH treatment (167.1 person-year) and 19 of 216 patients (8.8%) who did not receive INH treatment (427.9 person-year) had experienced LFT abnormalities. Among patients treated with INH (n = 96), baseline characteristics of patients who experienced LFT abnormality was also compared with patients who did not experienced LFT (Supplementary Table 1). Since INH treatment was significantly associated with LFT abnormality, we further investigated the association between INH treatment and the persistence of TNF inhibitors. TNF inhibitor persistence did not differ between patients who did and did not receive INH treatment (log-rank test, p = 0.79) (Fig. 1A). When we analyzed the impact of INH treatment on the discontinuation of TNF inhibitors due to adverse events (AEs), the INH treatment group did not show a higher TNF inhibitor discontinuation rate than those in the no INH treatment group (log-rank test, p = 0.37) (Fig. 1B). Among patients treated with INH (n = 96), TNF inhibitor persistence did not differ between patients who did and did not experience LFT abnormality (Supplementary Fig. 1).
In multivariate Cox proportional hazards analysis, INH treatment for LTBI (OR, 1.01; 95% CI, 0.66 to 1.57) was not a risk factor for discontinuation of TNF inhibitors, while longer disease duration (OR, 0.96; 95% CI, 0.93 to 0.99) and a history of liver function abnormality before starting TNF inhibitors (OR, 0.32; 95% CI, 0.13 to 0.82) were protective factors for discontinuation of TNF inhibitors in RA patients (Table 3).
DISCUSSION
In this study, we found that 12.5% of RA patients who started TNF inhibitors experienced LFT abnormality during a mean observational period of 22.9 months. Although INH treatment was a risk factor for LFT abnormality, it was not a risk factor for discontinuation of TNF inhibitors. This suggests that LFT abnormality caused by INH treatment of LTBI is appropriately controlled in clinical practice.
Our study showed a slightly higher incidence of LFT abnormality in patients treated with TNF inhibitors, compared to the 5.4% in a previous report [11]. This higher rate of LFT abnormality may be explained by several reasons. Firstly, our definition of LFT abnormality was any increase in LFTs above the normal range, or a patientŌĆÖs report that they had abnormal LFTs. Since many patients had LFTs checked between each visit to the rheumatology clinic, we included patient-reported LFT abnormality in our outcomes. Secondly, the higher rate of INH treatment among Korean TNF inhibitor users was another reason for the increased rate of LFT abnormality. In our study, about 30% of TNF inhibitor users were treated with INH with starting each agent. This may be related to the higher positive rate of LTBI screening tests in Korea compared with Western countries [12-16]. Therefore, this safety issue regarding INH treatment in TNF inhibitor users is more important in countries with a higher incidence of TB or LTBI than Western countries.
Several studies have reported that INH treatment for LTBI increases liver enzyme concentrations. One study reported that among 13 RA patients with a positive LTBI test or chest X-ray, eight patients were treated with INH and four patients (50%) experienced mild to severe hepatic dysfunction. The authors suggested that the incidence of hepatotoxicity due to INH is higher in RA patients treated with MTX or sulfasalazine and TNF inhibitors [8]. On the contrary, another study reported that 11% of 44 patients who used INH combined with MTX showed transient increases in LFT, but in no case was this more than twice the ULN values. Moreover, all abnormal LFTs resolved spontaneously without intervention [9]. However, previous studies did not show the exact impact of INH treatment on the occurrence of LFT abnormality or drug persistence of TNF inhibitors because of their small sample size as well as the absence of a control group.
LFT abnormality is a common AE in RA treatment and its occurrence is dependent on not medications but on sociodemographic factors and the combined comorbidities of each patient; therefore, direct comparison between studies is quite difficult. Therefore, to identify the exact impact of INH treatment on LFT abnormality, we selected patients with some criteria from the retrospective RESEARCh database and analyzed them with a case-control design. We selected patients who started TNF inhibitors and had an available DAS28 score, because initial disease activity might influence combination treatment with MTX or other DMARDs. To identify the effect of INH treatment on LFT abnormality, we divided patients according to LFT abnormality. In multivariable analysis, INH treatment for LTBI as well as male sex and high initial disease activity were risk factors for LFT abnormality in RA patients. Interestingly, MTX was protective for the occurrence of LFT abnormality. This result can be explained by channeling bias; physicians do not prescribe MTX for patients who are at high risk for LFT abnormality. In clinical practice, MTX can be stopped for TNF users with a high risk of LFT abnormality, but the use of INH for LTBI treatment is inevitable. Therefore, in clinical practice, INH might be a stronger risk factor for LFT abnormality than MTX in RA patients who use TNF inhibitors.
In spite of the independent risk of INH treatment on the occurrence of LFT abnormality, we found that the severity of these abnormalities was relatively low. According to the US Food and Drug Administration guidance for potential drug-induced liver injury from therapeutic agents, close observation should be performed in cases with symptoms or repeat testing that shows LFT > 3 ├Ś ULN or 2-fold increases above baseline values for subjects with elevated values before drug exposure [17]. Therefore, most patients with LFT abnormality were not required to stop RA treatment or LTBI treatment, although one patient stopped TNF inhibitor and LTBI treatment due to elevated LFT.
Our second objective was to identify the impact of INH treatment on the drug persistence of TNF inhibitors in RA patients, which we investigated due to the availability of many potential clinical decisions in practice. Firstly, MTX dosage should be lowered in patients who experience elevated LFTs due to INH treatment, though this might be increase the non-response rate of TNF inhibitors. Secondly, in Korea, there are strict guidelines for INH treatment of LTBI. INH treatment must be started at least 3 weeks before starting TNF inhibitors and should be continued for 9 months after starting TNF inhibitors. If INH treatment is not tolerable for patients with LTBI, regimens of LTBI treatment or anti-RA treatment should be altered. Thirdly, adverse effects of INH treatment including LFT abnormality can affect compliance with TNF inhibitors in some patients. Therefore, we hypothesized that LFT abnormality caused by LTBI treatment can directly influence TNF inhibitor persistence.
To determine the impact of INH treatment on the persistence of TNF inhibitors, we used a cohort design. We classified patients according to INH treatment and then performed survival analysis and Cox-proportional hazards analysis. The persistence of TNF inhibitors over 5 years was similar between the groups who did and did not receive INH treatment, and INH treatment was not a risk factor for discontinuation of TNF inhibitors. Since the major reasons for discontinuation of TNF inhibitors reported in previous studies are ineffectiveness of drug and occurrence of AEs such as infections and allergic reactions, we further analyzed the impact of INH treatment on the discontinuation of TNF inhibitors due to AEs, but there was no difference between the two groups.
Our analysis has some limitations. We did not collect information about alcohol intake or herbal or alternative remedies that can potentially cause liver function abnormality. However, since the decision to begin INH is dependent on the LTBI screening test result, which is not influenced by the above personal history, we hypothesized that those baseline characteristics would be evenly controlled in the two groups by the large sample size of our study. The other limitation is that the LFT testing was not performed as regularly as it is in randomized clinical trials. However, some patients might have regular laboratory tests performed at a private clinic or hospital for their comorbid conditions. Hence, we included the patient-reported history of LFT elevation between visits to our hospital as an outcome to avoid underestimating the prevalence of LFT abnormality.
In summary, INH treatment for LTBI in RA patients who used TNF inhibitors was associated with a high incidence of LFT abnormality, but did not affect the persistence of TNF inhibitors. This result should be emphasized for TNF inhibitor users, especially in countries with high positivity of LTBI screening tests. Additional studies are warranted to determine the optimal interval of LFTs and to develop a liver function monitoring strategy.
KEY MESSAGE
1. This study presented the usage and safety of isoniazid (INH) treatment for latent tuberculosis infection (LTBI) in tuberculosis endemic area, Korea.
2. Patients with non-DAD-ARDS were more likely to have therapeutic alterations based on histopathologic results. However, this did not lead to a significant improvement in the mortality rate.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





