


INTRODUCTION
Congestive heart failure (CHF) is becoming a major worldwide public health problem that requires a global response and enhanced survival after coronary artery disease, congenital or valvular heart disease, and societal aging. CHF is a complex clinical syndrome in which the heart cannot pump sufficient blood to the body. Various diseases or noxious stimuli, such as myocardial ischemia, high blood pressure, tachycardia, inflammation, or excess neurohormonal stimulation comprise the pathophysiological mechanisms of CHF. Significant strides have been made in the treatment of CHF by neurohormonal modulation using angiotensin-converting enzyme inhibitors, angiotensin-II receptor blockers, ╬▓-blockers, and aldosterone antagonists [1]. However, 1-year mortality in clinical trials remains high and exceeds 6% in patients with CHF and mild to moderate symptoms [2] and 12.8% in patients with CHF and moderate to severe symptoms [3], warranting further strategies to reduce adverse outcomes. 3-Hydroxy-3-methylglutaryl coenzyme A reductase inhibitors or statins are candidate drugs that have been investigated and used in patients with CHF.
It is well-established that statins reduce morbidity and mortality in patients with coronary artery disease, thus preventing its progression to CHF [4], and have cholesterol-independent pleiotropic effects by inhibiting mevalonate. Statins decrease isoprenoid production and consequently downregulate the inflammatory pathways mediated by Rho proteins [5] and reactive oxygen species generated by Rac proteins [6]. Additionally, many observational studies and retrospective and post hoc analyses of data from randomized trials of patients with various cardiovascular conditions suggest the survival benefit of statins in patients with CHF [7,8,9]. However, two large randomized controlled trials suggested that statins do not benefit patients with heart failure. The Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA) [10] and Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardio-Heart Failure (GISSI-HF) [11] randomized patients to rosuvastatin or a matching placebo and evaluated long-term outcomes in patients with CHF. Regrettably, neither study showed improved survival in patients with CHF. However, recent studies have not confirmed the detrimental effects of statins in CHF patients reported in the CORONA and GISSI-HF trials [12,13]. Therefore, the effect of statins on patients with CHF is not clear, raising important clinical questions. In particular, concerns have been raised about potential adverse effects (AEs) of high-dose statin therapy [14], because observational studies have detected an association between low cholesterol levels and adverse outcomes in CHF patients [15]. A hypothesis was proposed that the decrease in ubiquinone levels caused by statin therapy may have deleterious consequences, because ubiquinone is a potential antioxidant and a key molecule in mitochondrial function and, thus, muscle strength [16,17].
Pitavastatin is a lipophilic statin with longer-acting cholesterol lowering effects than that of other statins. Pitavastatin also has high bioavailability and is minimally metabolized by the cytochrome P450 system [18,19]. The South koreAn Pitavastatin Heart FaIluRE (SAPHIRE) study was designed to randomize patients with CHF due to New York Heart Association functional class II to III ischemic heart disease into low potency, hydrophilic, 10 mg pravastatin or high potency, lipophilic, 4 mg pitavastatin daily groups and to evaluate systolic function and exercise capacity changes after 1 year.
METHODS
Study population
This was a prospective, randomized, open label, active drug-controlled, and two parallel group-comparison study to evaluate the efficacy and safety of pitavastatin compared with pravastatin in patients with chronic ischemic heart failure. Clinically stable (NYHA class II to III) male and female patients with heart failure (age, 30 to 80 years), with a left ventricular ejection fraction (EF) Ōēż 45% and serum low density lipoprotein cholesterol (LDL-C) Ōēź 70 mg/dL at screening, were enrolled. Patients were excluded if they had any of the following conditions: decompensated heart failure (NYHA class IV), acute myocardial infarction, unstable angina, coronary artery bypass graft, percutaneous coronary intervention or valve surgery within 3 months, uncontrolled heart failure due to hypertrophic obstructive cardiomyopathy, mild-to-severe valvular stenosis, or severe (grade III/IV) valvular regurgitation. Female patients with child-bearing potential and pregnant and nursing women were excluded. This study was approved by the Institutional Review Board and the Korea Food and Drug Administration and was conducted in accordance with Korean Good Clinical Practice and the Declaration of Helsinki. This study has been registered at Clinical-Trials.gov (ID; NCT00701285). All patients signed written informed consent prior to participation.
Study design
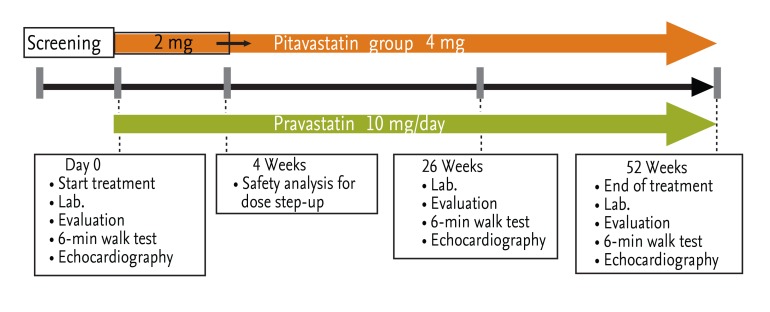
The clinical trial was conducted at five clinical research centers and hospitals. All patients provided written informed consent prior to participation. Subjects who satisfied all inclusion/exclusion criteria were randomized either to the pravastatin group or the pitavastatin group. The pravastatin group was administered 10 mg pravastatin once daily and the pitavastatin group 2 mg pitavastatin once daily. If no AEs were determined by the investigators after 4 weeks, the pitavastatin dose was doubled to 4 mg once daily regardless of the serum cholesterol level, and the patients were treated for 52 weeks. The study design is summarized in Fig. 1.
Patient compliance and the presence of AEs, regardless of an association with the study drugs, were evaluated at each visit by direct interview using a prespecified script and pill counts. Blood samples were collected to evaluate any changes during the administration of the study medications.
All laboratories in the hospitals that participated in this study used procedures that were in accordance with the guidelines of the Clinical and Laboratory Standards Institute for sample collection and handling. They regularly participated in proficiency tests and were accredited by the Korean Association of Quality Assurance for Clinical Pathology.
Clinical follow-up
The duration of the study was 52 weeks. Left ventricular dimensions and ejection fraction (EF) were measured at baseline and 52 weeks after initiating statin therapy using the modified Simpson's method. The patients also underwent the 6-minute walk test at baseline and 6 months after initiating statin therapy. B-natriuretic peptide (BNP) levels were compared at baseline and 6 months after initiating statin therapy by one central laboratory.
Outcome
The primary endpoint was the composite outcome of heart failure aggravation including hospitalization due to heart failure and total deaths. Hospitalization due to heart failure was determined by the investigators. The secondary outcome was the change in echocardiographic EF after statin treatment. Secondary endpoints included functional assessments using the 6-minute walk test and NYHA class, left ventricular end-diastolic pressure evaluated by the E/e' ratio [20], and BNP levels [21]. Safety endpoints included an evaluation of AEs, vital signs, and clinically significant abnormal values among the laboratory test results throughout the study.
Statistical analysis
Since no previous reports have compared the effect of statins in patients with heart failure, a sample size of 35 patients per group was needed to detect a 20.0% difference in LDL reduction between the two groups with a standard deviation of 27.0%, 80% power to reach a p value of 0.05, and a drop-out rate of 20%. The statistical analysis was performed using SAS version 9.2 (SAS Institute, Cary, NC, USA). Results are expressed as means, standard deviations, and ranges for baseline data, including demographics, medical history, physical examinations, and drug history. All data were compared by an independent biostatistician using one-way analysis of variance (continuous variables) or the chi-square test (discrete variables). The change between baseline and the last observation carried forward value was compared with the paired t test. No adjustment was made for baseline covariates.
The overall rate and frequency of AE occurrence and the rate and frequency of AE occurrence that met the following categories were summarized by treatment group and compared between the two treatment groups using Fisher exact test: AEs whose causality to the study drug could not be ruled out, severely intense AEs, serious AEs, and AEs that led to discontinuing the study drug. The t test was used with a two-sided significance level of 5% to determine if there was any difference between the two groups with respect to the change from baseline to the end of the study.
RESULTS
Study population and baseline characteristics
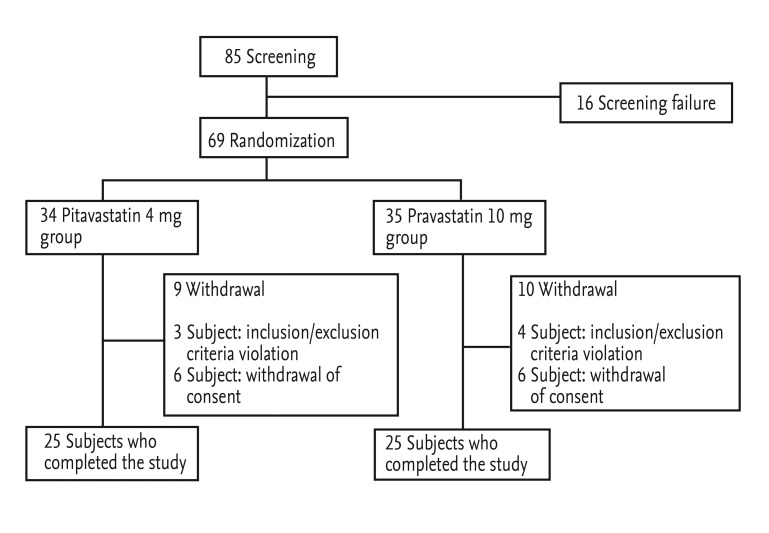
Of the 85 screened patients from six study institutions, 16 were excluded during screening, and 69 were randomized (34 to the pitavastatin group and 35 to the pravastatin group). Three subjects randomized to the pitavastatin group and four subjects randomized to the pravastatin group were excluded before administration of the study drugs, as they violated the inclusion/exclusion criteria and withdrew their consent to participate in this study. After administrating the study drug, six subjects in the pitavastatin group and six subjects in the pravastatin group withdrew; thus, 50 subjects (25 in the pitavastatin group and 25 in the pravastatin group) completed the study (Fig. 2). No significant difference was observed between the two groups for withdrawal rate (p = 0.833). Primary efficacy was analyzed in the intention-to-treat population (31 in the pitavastatin group and 31 in the pravastatin group), which included all subjects who received at least one dose of the study drug.
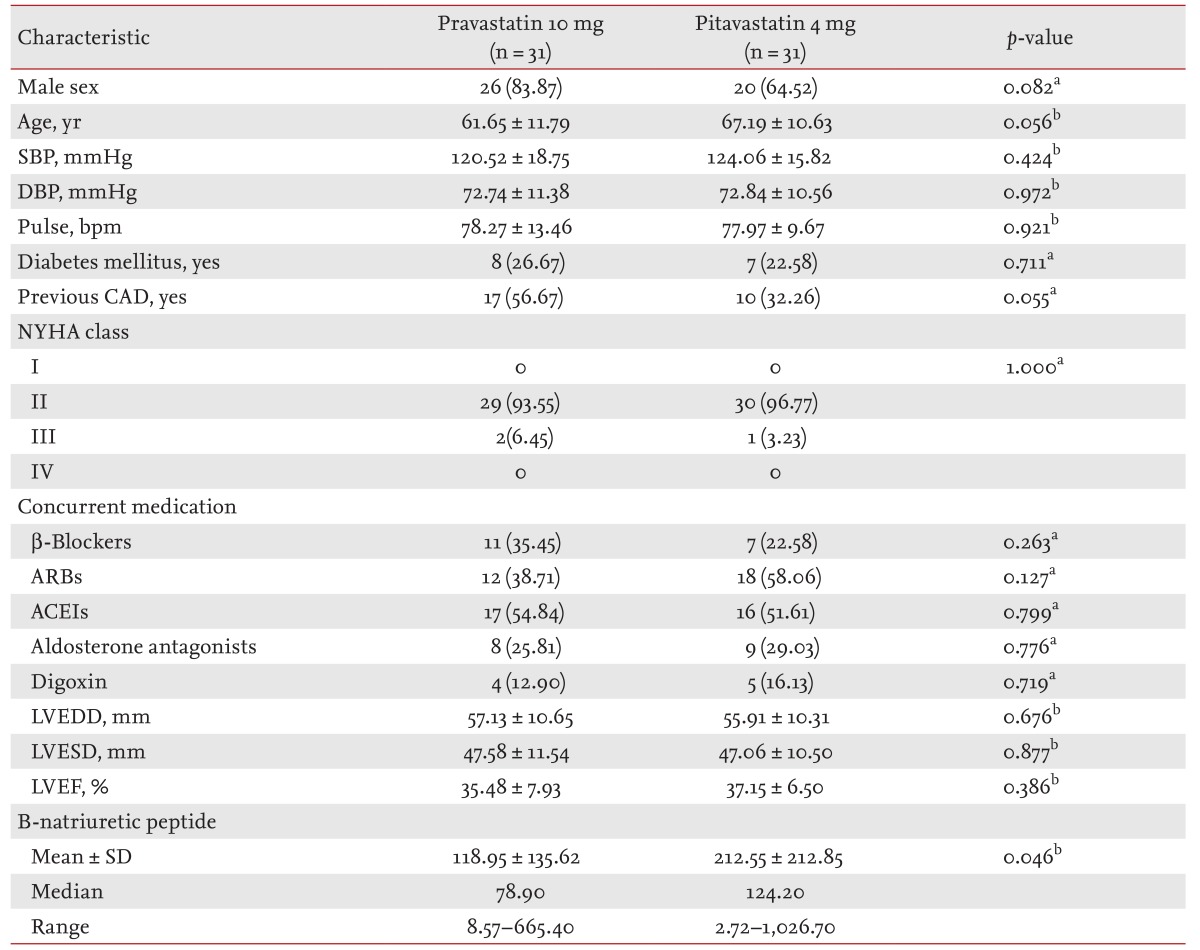
The majority of the patients were male (74%) with a mean age of 64.4 ┬▒ 11.5 years. Although the prevalence of males was higher in the pravastatin group (84%) compared with the pitavastatin group (65%), no statistical difference was detected (p = 0.082). The NYHA class distribution was 95% in class II and 5% in class III. The mean duration of CHF was 2.7 ┬▒ 3.7 years, and 48% of patients had a history of admission due to CHF; 24% of patients had diabetes mellitus, 64% had a history of myocardial infarction, and 57% had undergone coronary revascularization (percutaneous intervention 53%, coronary artery bypass graft 7%). Baseline patient characteristics did not differ between the groups (Table 1).
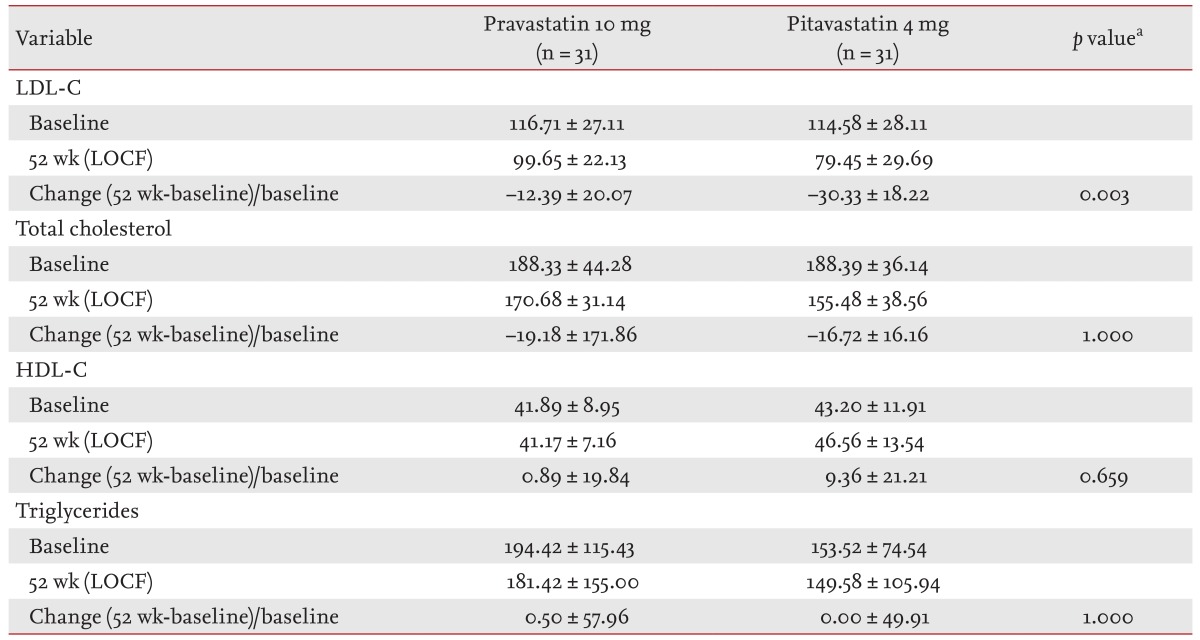
Change in lipoprotein values
LDL-C decreased significantly by 30% in the 4 mg pitavastatin group, from a mean of 114.58 to 79.45 mg/dL (p < 0.001). The reduction in LDL-C in the pitavastatin group was significantly greater than the 12% reduction in the 10 mg pravastatin group (p = 0.003).
Total cholesterol levels decreased significantly by 16% in the 4 mg pitavastatin group (p < 0.001) and by 19% in the 10 mg pravastatin group (p = 0.016). Although the extent of cholesterol reduction was greater in the pitavastatin group, no statistical difference was observed.
The HDL cholesterol level was increased by 9% in the 4 mg pitavastatin group with borderline significance (p = 0.052); however, no change was observed in the pravastatin group (p = 0.635). Triglyceride levels remained unchanged in both groups. The changes in cholesterol and lipoprotein levels are summarized in Table 2.
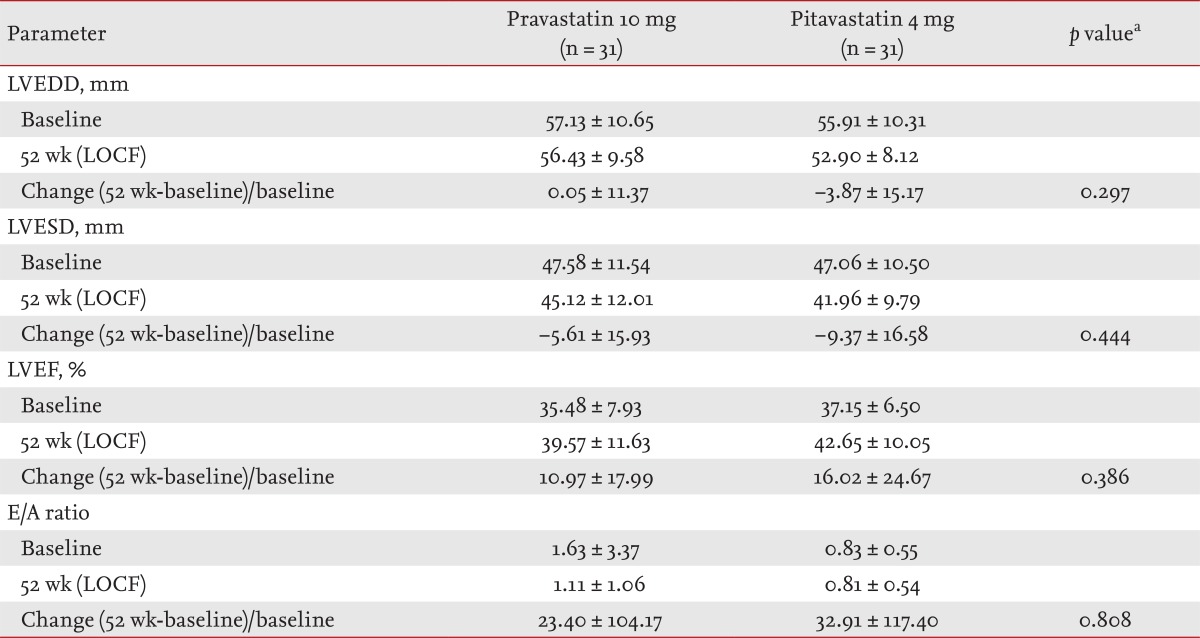
Left ventricular remodeling following statin treatment
The left ventricular systolic dimensions decreased significantly by 9% in the pitavastatin group (p = 0.011) and by 5% in the pravastatin group (p = 0.026). The difference between the two groups was not significant (p = 0.444) (Fig. 3A).
EF improved significantly from 37% to 42% in the pitavastatin group (p = 0.003) and from 35% to 39% in the pravastatin group (p = 0.002). Although the extent of the EF change was greater in the pitavastatin group (16% vs. 11%), no statistical difference was observed between the groups (p = 0.386) (Fig. 3B).
In contrast, left ventricular diastolic function, evaluated by the E/A ratio, remained unchanged in both groups (p = 0.88) (Fig. 3C). The left atrial diameter also remained unchanged (data not shown). The changes in left ventricular dimensions and systolic and diastolic function evaluated by echocardiography are summarized in Table 3.
Exercise capacity, BNP changes, and outcomes following statin treatment
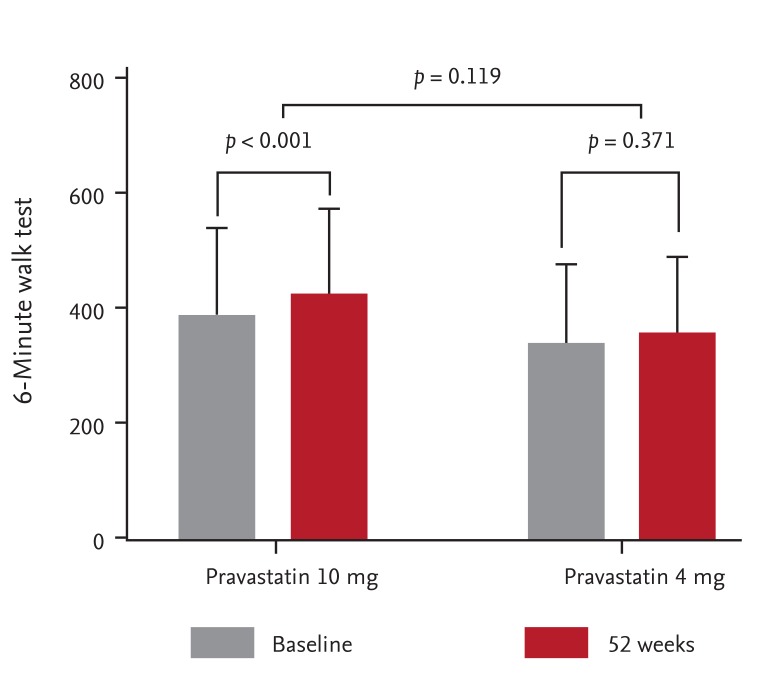
Exercise capacity evaluated by the 6-minute walk test improved significantly in the 10 mg pravastatin group (p < 0.001), however, no change was observed in the pitavastatin group (p = 0.371) (Table 4, Fig. 4). More patients (n = 4) in the pravastatin group tended to show an improved NYHA class than those in the pitavastatin group (n = 2). BNP levels did not change significantly in either group.
No mortalities were observed during the 1-year treatment period. One patient in the pitavastatin group was admitted due to aggravated heart failure after 207 days of treatment. Two patients in the pravastatin group were admitted due to heart failure: one patient after 157 days and the other after the treatment phase ended (455 days).
Tolerability
No AE was reported before administration of the investigated products. Thirteen subjects (40%) in the pitavastatin group and 12 subjects (36%) in the pravastatin group experienced an AE; however, no treatment-related AEs were found in either group by the investigators. None of the laboratory parameters differed between the groups (data not shown).
DISCUSSION
The SAPHIRE study investigated the dose-effect relationship of statins in patients with ischemic CHF. Since no previous data on the dose-effect relationship among the extremely different doses/potencies of statins in CHF patients are available, this exploratory study was initiated with 35 patients enrolled per group as a baseline LDL-C-lowering efficacy trial. Due to the small sample size, our findings suggested two hypotheses regarding the effect of statins in patients with CHF. First, low dose, low potency pravastatin lowered LDL-C by 12%, and high dose, high potency pitavastatin lowered LDL-C by 30%. Both treatments improved left ventricular systolic function after 1 year, suggesting that these statins might have beneficial cardiac remodeling effects in patients with ischemic CHF. Second, in contrast to improved cardiac systolic function, high dose, high potency pitavastatin did not improve exercise capacity or functional capacity in patients with CHF, although low dose, low potency pravastatin showed some beneficial effects on exercise capacity, suggesting that lowering cholesterol too much may not be beneficial for muscle strength.
Despite the molecular biological activities of statins, which clearly show anti-inflammatory and antioxidant effects, the results of two randomized trials evaluating rosuvastatin and one evaluating pitavastatin failed to show a reduction in cardiovascular events [10,11,22]. The CORONA study randomized 5,011 patients with ischemic CHF to 10 mg rosuvastatin or placebo [10]. The GISSI-HF trial randomized 4,631 patients with CHF of all etiologies to 10 mg rosuvastatin or placebo [11]. The rosuvastatin treatment did not affect the primary endpoints in the two studies and only showed a benefit for the number of CHF hospitalizations in the CORONA trial. However, it was unclear whether the results of the CORONA study and the GISSI-HF trial can be generalized to all patients with CHF or to the different kinds of statins. A meta-analysis reported that the effects of statins on CHF are not class effects, and a significant benefit was found using lipophilic atorvastatin but not hydrophilic rosuvastatin [23,24]. However, a third randomized trial on lipophilic pitavastatin, the PEARL study, also failed to show benefits [22], which strongly suggests that the effects of statins on CHF are class effects.
Although it is still debated whether statins cause fatigue, thus, limiting exercise capacity, one study showed that even statins with modest potency, such as simvastatin and pravastatin, contribute to significant AEs on energy and fatigue with exertion [25]. A post hoc analysis of the CORONA study also reported a small but significant worsening of fatigue in older patients with systolic heart failure [26]. Myopathy, a rare but well-reported AE of statins, clearly increases with high-dose statin use compared with lower dose, low potency statin use [25,27], which may explain our findings. Another explanation regarding statin-related fatigue is that statins may increase the perception of fatigue through a central nervous system effect, and lipophilic statins increase this perception more than that of hydrophilic agents such as rosuvastatin [28].
Other hypotheses arguing against statin treatment in CHF patients are the endotoxin lipoprotein hypothesis, the coenzyme Q10 (ubiquinone) hypothesis, and the selenoprotein hypothesis [29]. In particular, the endotoxin lipoprotein hypothesis is related to lower cholesterol levels. Several studies have addressed the relationship and relevance between serum cholesterol level and outcomes in patients with CHF and consistently suggested that too low of cholesterol levels are associated with increased mortality [15,30].
The findings of the SAPHIRE study are quite interesting, showing that pravastatin and pitavastatin may have a beneficial cardiac reverse remodeling effect and may improve systolic function regardless of potency and lipophilicity/hydrophilicity. The absolute extent of the benefit was greater with the more potent pitavastatin, although no statistical significance was observed, mainly due to the small sample size. In contrast, high dose, high potency pitavastatin failed to improve exercise capacity or functional capacity in patients with CHF, although low dose, low potency pravastatin showed some beneficial exercise capacity effects. These findings may offer a new hypothesis that statin therapy is beneficial for cardiac reverse remodeling, at least in patients with ischemic CHF; however, the adequate dose and potency to maximize the effect must be determined.
Our findings should be considered in the context of several limitations. This study was designed as an exploratory study and enrolled a small number of patients. Therefore, a larger and longer duration study is warranted to confirm our findings. Second, we tried to narrow the scope to patients with ischemic CHF and to maximize the potency, dose, and characteristics of the statins due to the small sample size. Therefore, our findings cannot be generalized to all patients with CHF unless supported by further studies. Last, although low potency pravastatin may improve exercise capacity, we did not observe significant hemodynamic, echocardiographic, or BNP changes associated with CHF symptoms. Therefore, uncertainty remains as to whether a low dose statin is beneficial for exercise capacity.
In conclusion, both low dose pravastatin and high dose pitavastatin had a beneficial cardiac reverse remodeling effect and improved systolic function in patients with ischemic CHF. However, only low dose pravastatin improved exercise capacity significantly. These findings suggest that "too much" lowering of cholesterol might not be beneficial for functional capacity in patients with CHF.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





