


To the Editor,
Sarcoidosis is a systemic granulomatous disorder of unclear etiology that affects the lungs, eyes, skin, heart, and other organs [1]. Subcutaneous sarcoidosis occurs less frequently and is seen in approximately 12.2% of Asian patients with sarcoidosis [2]. Subcutaneous sarcoidosis is characterized by an insidious onset of multiple small subcutaneous nodules that are commonly located on the extremities (78.8%), trunk, face, and groin [3]. Although subcutaneous sarcoidosis is strongly associated with systemic disease, severe hypercalcemia, and acute kidney injury (AKI) are rarely reported [3,4]. We herein report a case of subcutaneous sarcoidosis presenting as a large, fixed suprapubic mass mimicking malignancy. The case was complicated by severe hypercalcemia and AKI, and it did not involve the lungs.
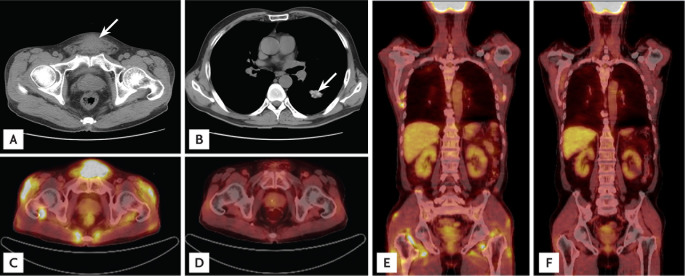
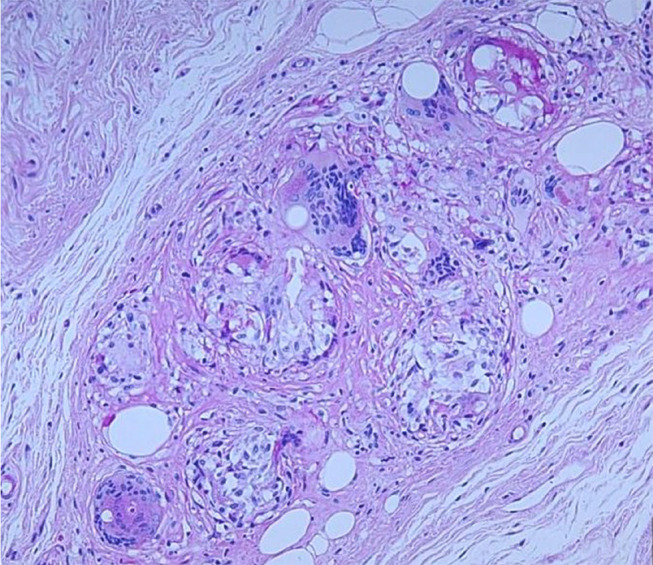
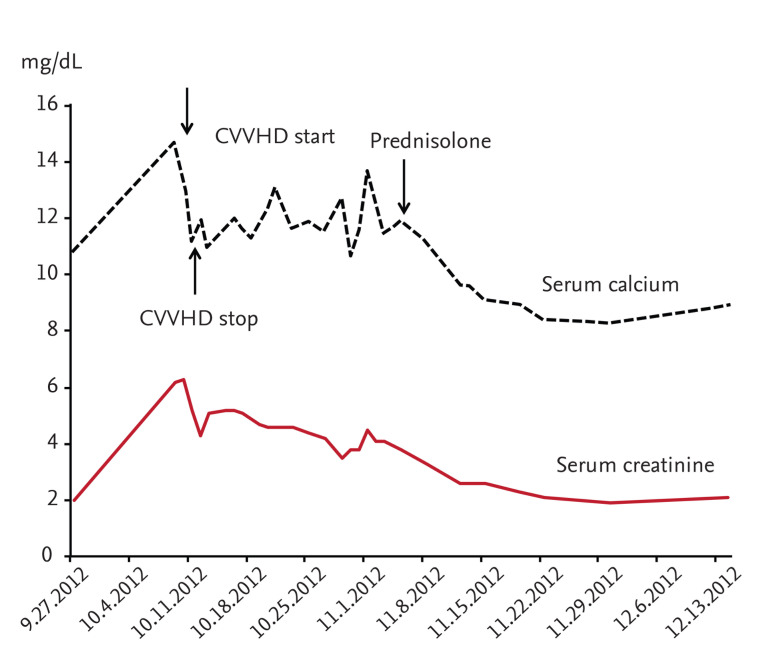
A 61-year-old Korean man presented to the hospital with a progressively enlarging suprapubic mass. He had been diagnosed with diabetes mellitus and hypertension 10 years previously. Two years before admission, he was diagnosed with membranous nephropathy and treated with cyclosporine and prednisolone. At that time, his creatinine (Cr) level was 1.53 mg/dL. A physical examination revealed a firm, nontender, round, fixed mass without skin lesions in the suprapubic area. There was no palpable lymphadenopathy or hepatosplenomegaly. Initial laboratory findings showed serum Cr and serum calcium (Ca) levels of 2.0 and 11.0 mg/dL, respectively. After 12 days, the serum Cr and Ca levels increased to 6.2 and 14.7 mg/dL, respectively. Other laboratory results were as follows: serum level of blood urea nitrogen, 55.9 mg/dL; ionized Ca, 1.91 mmol/L (reference range, 1.13 to 1.32); phosphorous, 4.5 mg/dL; intact parathyroid hormone, 8.1 pg/mL (reference range, 14 to 72); serum alkaline phosphatase, 47 IU/L (reference range, 42 to 128); 1,25-dihydroxyvitamin D, 71.2 pg/mL (reference range, 25.1 to 66.1); parathyroid hormone related peptide, < 1.1 pmol/L; angiotensin-converting enzyme, 110.2 U/mL (reference range, 9 to 47); thyroid-stimulating hormone, 0.706 µIU/mL; hemoglobin, 12.1 g/dL; white blood cell count, 9.8 × 103/µL; platelet count, 370 × 103/µL; urine Ca/Cr ratio, 303 mg/g; and 24-hour urine protein, 312.8 mg/day. Abdominal computed tomography (CT) revealed a 4.4 × 3.3-cm suprapubic mass in the subcutaneous area (Fig. 1A). A chest CT scan showed did not show hilar lymphadenopathy (Fig. 1B). 18F-fluorodeoxyglucose positron emission tomography/CT (18F-FDG PET/CT) showed multiple foci of hypermetabolic activity in the suprapubic area, both shoulders, flank, hip, and thigh, and there were no hypermetabolic lesions in the lung (Fig. 1C and 1E). He was treated with intravenous fluids, furosemide, bisphosphonate, calcitonin, and renal replacement therapy (continuous venovenous hemodialysis). However, his Ca and Cr levels were persistently elevated at 11.0 and 5.1 mg/dL, respectively. The suprapubic mass was excised and histologically identified as noncaseating granulomatous inflammation within fat tissue. The solid granuloma was composed of epithelioid histiocytes and multinucleated giant cells engulfing fat vacuoles and mild lymphocytic infiltration (Fig. 2). The patient was started on oral prednisolone 30 mg/day, and his Ca level decreased to 9.6 mg/dL after 1 week of treatment. After 2 weeks, his Cr level improved to 2.3 mg/dL (Fig. 3). Prednisolone was slowly tapered off over 3 months. After 3 months of treatment, a follow-up 18F-FDG PET/CT scan demonstrated complete resolution of the multiple hypermetabolic lesions (Fig. 1D and 1F), and his Cr and Ca levels were 2.0 and 8.8 mg/dL, respectively. His renal function and serum Ca levels remain stable after 1 year of treatment. The subcutaneous sarcoidosis associated with hypercalcemia and AKI was successfully treated with a moderate dose of prednisolone.
Subcutaneous sarcoidosis is observed in 2% to 12% of patients with systemic sarcoidosis [2,3]. It presents with insidious onset of multiple, nontender, firm, mobile, and round subcutaneous nodules. The lesions vary from 1 to 100 in number and from 0.5 to 2.0 cm in size; the skin lesions are usually asymptomatic. The lesions are mainly distributed in the extremities (76% to 100%), followed by the trunk (28%), buttocks (10%), and forehead (5%) [3]. Subcutaneous sarcoidosis is frequently associated with systemic diseases such as bilateral hilar lymphadenopathy (94%), arthritis (19%), peripheral neuropathy (13%), renal involvement (13%), and uveitis (13%) [3].
In this case, the patient presented with a single large mass in the suprapubic area. There was no bilateral hilar lymphadenopathy or palpable lesion other than the suprapubic mass. Additionally, the patient showed severe hypercalcemia and AKI, which is a rare presentation of subcutaneous sarcoidosis [4]. Malignancies such as lymphoma and soft tissue sarcoma were considered as differential diagnoses. The diagnosis of subcutaneous sarcoidosis was based on the patient's clinical and radiological findings and supported by the histopathological findings of a noncaseating epithelioid granuloma predominantly involving panniculus with minimal inflammation and without evidence of organisms or exogenous particles [1,3]. The sarcoidosis was characterized by infiltration of CD4 type 1 helper cells and macrophages into the sites of inflammation, and these cells increased the 18F-FDG uptake [5]. 18F-FDG PET/CT scans showed good sensitivity (87%) in detecting all biopsy-proven sarcoidosis localizations excluding skin involvement [5]. 18F-FDG PET/CT revealed multiple sites of involvement in the subcutaneous and muscle layers at the time of diagnosis, and complete resolution of the lesions was seen after the prednisolone treatment. 18F-FDG PET/CT was useful in evaluating the extent of disease and follow-up response to therapy in this patient.
Hypercalciuria is the most common abnormality of Ca metabolism in sarcoidosis, ranging from 40% to 50% [1]. Although hypercalcemia occurs in 7.4% to 11.0% of patients, clinically significant hypercalcemia is less common, with a prevalence of < 5% of patients [1,5]. However, hypercalciuria was not present despite the severe hypercalcemia in this patient. An increased plasma 1,25-dihydroxyvitamin D level is a probable cause of hypercalcemia, and macrophages in patients with sarcoidosis contain 25-hydroxyvitamin D-1α-hydroxylase, which converts 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D [1].
Corticosteroids are the drugs of choice to decrease the endogenous production of 1,25-dihydroxyvitamin D [1,3]. Oral prednisolone at 20 to 40 mg/day has been suggested as the initial treatment dose for sarcoidosis, and this can be reduced over a period of 1 to 3 months [1]. Evidence supporting the use of immunosuppressive agents such as methotrexate is currently lacking.
In summary, we have reported a patient with subcutaneous sarcoidosis who presented with a suprapubic mass, hypercalcemia, and AKI and was successfully treated with a moderate dose of prednisolone.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





