


INTRODUCTION
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium tuberculosis. It typically affects the lungs but can affect other sites. TB is one of the leading causes of mortality and morbidity worldwide. In 2010, there were 8.8 million cases of TB, 1.1 million deaths from TB among human immunodeficiency virus (HIV)-negative people, and an additional 0.35 million deaths from HIV-associated TB [1]. Despite rapid economic development in South Korea, TB remains an important health issue in the country. Nationwide, 33,167 TB cases were reported in 2010. The prevalence and annual incidence of TB in South Korea are currently estimated to be 151/100,000 and 97/100,000, respectively [1].
Indoor air pollution is a well-known risk factor for TB development. The association between indoor air pollution and TB was suggested as early as 1911. Observations between 1858 and 1902 in Paris that TB mortality was inversely associated with the number of windows per household were the first suggestion of a connection [2]. Since then, many studies showing an association between indoor air pollution and TB have been published. For example, among residents of Mexico City, cooking with a biomass stove was associated with a 2.4-times higher odds of developing TB [3]. One recent meta-analysis showed that indoor air pollution increased the incidence of pulmonary TB, with a relative risk (RR) of 1.95 [4].
Despite the well-established relationship between indoor air pollution and TB, the impact of outdoor air pollution on the development of TB has not been examined sufficiently. We assessed the impact of major air pollutants on TB development in the Seoul metropolitan area, South Korea, an intermediate TB burden country.
METHODS
Study design
The study protocol was approved by the Institutional Review Board (IRB) of Seoul National University Hospital. Because this study was performed retrospectively using anonymous data, obtaining informed consent from individual patients was waived by the IRB.
This was a retrospective cohort study involving the entire population of the Seoul metropolitan area. After adjusting for socioeconomic status, the mean concentrations of ambient particulate matter (PM) with an aerodynamic diameter Ōēż 10 ┬Ąm (PM10), O3, CO, NO2, and SO2 between January 1, 1997 and December 31, 2006, were tested as risk factors for the development of TB in Seoul between January 1, 2002 and December 31, 2006.
Population data
Mid-year population data for each year, grouped in 5-year age bands, for each of the 522 Seoul metropolitan area townships were obtained from the National Statistics Office [5]. For township-level socioeconomic status, deprivation indices using the Carstairs Index [6] were assayed for each townships across Seoul. Specifically, we analyzed the township-specific 1) proportion of overcrowded households (more than 1.5 persons/room), 2) percent of unemployment among males between 15 and 64 years, 3) percentage in manual occupations, and 4) lack of car ownership, based on 2005 National Census data. Finally, we generated a township-specific deprivation index by averaging the standardized z-scores for the four census-derived indicators. Subsequently, the townships were classified into five quintiles, based on the deprivation level.
Air pollution exposure estimate
Measurement of air pollutants were obtained from 27 monitoring stations, evenly scattered throughout Seoul and maintained by the Department of the Environment, through the period from January 1, 1997 to December 31, 2006. Each monitoring station provided hourly readings of PM10, O3, CO, NO2, and SO2 concentrations. Using the data from each monitoring station, we estimated the pollutant levels in each township using the ordinary kriging method [7]. We used the Spatial Analyst and Geospatial Analyst extensions of ArcGIS (ArcMap version 9.3, ESRI Inc., Redlands, CA, USA) using 1 ├Ś 1 km grids to partition each township for each pollutant. We extracted the concentrations of each pollutant using the central point of the kriging map for each township.
TB incidence
In Korea, physicians who diagnose TB in patients must report this electronically immediately to the Korean Institute of Tuberculosis [8]. The reporting form includes demographic information (e.g., age, gender, address) and clinical characteristics (e.g., past history of TB treatment, site of TB, smear positivity) of TB patients. Annual numbers of reported TB cases in each township were retrieved from that database. Incidences of township TB were calculated from the annual number of TB cases divided by the mid-year population of each township.
Statistical analyses
We calculated standardized incidence ratios (SIRs) for each township using data from January 1, 2002 to December 31, 2006. Expected cases were determined by multiplying the gender- and age-specific TB incidences in 5-year age bands by the corresponding gender- and age-specific population-years at risk in each township. The statistical assumption underlying these estimates is that the observed disease (i.e., TB) counts, yi, in each town area arise from a Poisson distribution with mean riEi, where Ei is the age- and gender-standardized expected number of TB cases in town area i and ri is the RR of disease in that area.
We used a hierarchical Bayesian method to estimate the pollution-specific RR of TB for each gender, adjusted for area deprivation level, using the intrinsic Gaussian conditional autoregressive model. This model controls the spatial autocorrelation component. Relative rates were estimated using Markov Chain Monte Carlo algorithms [9] with WinBUGS version 1.4.3 (MRC Biostatistics Unit, Cambridge, UK), which was called from 'R' version 2.12.0. Parameter means and 95% credible intervals (CrIs) were calculated from five independent chains of 50,000 iterations after a burn-in of the first 20,000 iterations. The convergence of posterior distribution was assessed with the Gelman-Rubin convergence diagnostic [10], and models were compared based on the deviance information criterion.
RESULTS
Air pollutant concentrations
Descriptive statistics for the air-quality variables are presented in Table 1. The average concentrations were 63.5 ┬Ąg/m3 particulate matter (PM10), 16.0 ppb ozone (O3), 77.4 ppb carbon monoxide (CO), 34.4 ppb nitrogen dioxide (NO2), and 6.1 ppb sulfur dioxide (SO2). Of these, the annual averages of PM10 and NO2 were higher than the Korean national standard (PM10 Ōēż 50 ┬Ąg/m3 and NO2 Ōēż 0.03 ppm) [11].
Numbers and characteristics of TB cases
Between January 1, 2002 and December 31, 2006, in Seoul, a total of 41,185 TB cases were reported to the Korean Institute of Tuberculosis. Of these, 24,952 (60.6%) were males. The mean age of the male patients was 44.2 years, and that of the female patients was 41.9 years. Of the male patients, 21,048 (84.4%) were new cases with no past history of TB treatment. Of the females, 14,547 (89.6%) were new cases. The proportion of smear-positive TB was 36.8% in males and 29.6% in females (Table 2).
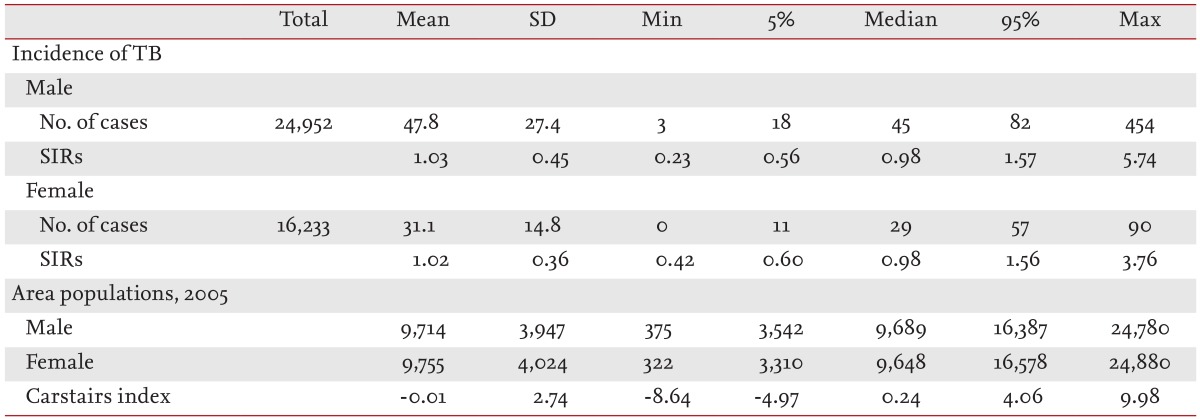
The mean male population of each township in 2005 was 9,714 and the mean female population was 9,755. The mean incidence of TB among males in each township was 47.8 and that of females was 31.1. Average SIRs of 522 Seoul metropolitan area towns were calculated as 1.03 for males and 1.02 for females (Table 3).
Impact of air pollutant concentration on TB incidence
PM10, O3, CO, and NO2 concentrations were not associated with the incidence of TB in males or females. However, the interquartile increase in SO2 concentration was associated with a 7% increase in TB incidence (RR, 1.07; 95% CrI, 1.03 to 1.12) in males but not females (RR, 1.02; 95% CrI, 0.98 to 1.07) (Table 4).
Geographic distribution of air pollutants and incidence of TB
Fig. 1 provides a map of the Seoul metropolitan area and the SO2 krigged values between January 1, 1997 and December 31, 2006, using 27 monitoring stations, categorized by deciles. The predicted SO2 concentrations of the central and northern townships were higher than those of other areas. Fig. 2 shows the unsmoothed and smoothed geographical distribution of the incidence of TB in males and females for the period January 1, 2002 to December 31, 2006. There was no spatial cluster of TB incidence; however, the incidence in the southern townships was generally higher than that in other areas.
DISCUSSION
Despite the established relationship between indoor air pollution and TB, the impact of outdoor air pollution on the development of TB has not been determined. In this study, by analyzing air pollutant data and formally reported TB cases, we found that annual SO2 level is associated with an increased risk of TB in males in the Seoul metropolitan area, South Korea, a country with an intermediate TB burden.
The group of air pollutants collectively termed "sulfur oxides" comprises both gaseous and particulate chemical species. Four gas-phase compounds of sulfur oxide exist (SO, SO2, SO3, and S2O). Among them, only SO2 is present at sufficient concentrations in ambient air to be a public health concern [12]. Because of its high water solubility, SO2 can be readily scrubbed from inhaled air in the upper airways [13]. Penetration is more efficient during oral, rather than nasal, breathing and during physical activity. Upon contacting airway-covering fluid, SO2 dissolves quickly into the aqueous phase. Subsequently, it readily dissociates into bisulfite and sulfite ions, which can be transferred into the systemic circulation [12,13].
SO2 can affect various aspects of the pulmonary defenses, including alveolar macrophage function, mucociliary transport, and alveolar clearance. In a previous study, in vitro exposure to 12.5 ppm SO2 for 30 minutes induced the death of 62% of alveolar macrophages and caused a 63% decrease in the release of reactive oxygen species [14], which probably play a significant role in intracellular inhibition/killing of mycobacteria [15]. Another study indicated that in vitro exposure to SO2 decreased production or release of tumor necrosis factor-╬▒ (TNF-╬▒) and interleukin-1 [16]. TNF-╬▒ is crucial for host defenses against M. tuberculosis because it plays a central role in the containment of tuberculous bacilli through granuloma formation [17]. Frequent reactivation of latent TB in patients using a TNF-neutralizing agent underscores the importance of TNF-╬▒ in defenses against M. tuberculosis [18]. Thus, the association between SO2 exposure and the development of active TB in our study may have been mediated by the negative effect of SO2 on reactive oxygen intermediate and TNF-╬▒.
In this study, an association between SO2 exposure and TB was observed only in males. This may be due to gender differences in susceptibilities to air pollutants as well as to TB. Indeed, epidemiological studies on the effects of air pollutants on respiratory health have shown significant gender differences [19]. For example, SO2 and PM2.5 had a greater effect on forced expiratory volume in 1 second in males (199 mL) than females (87 mL) [20]. In addition, the association between SO2 exposure and evening peak expiratory flow rate was observed only in boys with asthma [21]. Hypotheses explaining these differences include anatomical/physiological differences in the airway [22], gender-linked hormonal status [23], and other factors (more household tasks performed by females may result in increased exposure to viral infection, indoor allergens, combustion exhaust, cleaning solvents, and aeroallergens) [24].
Furthermore, males seem to be more affected by TB than females, with a male/female ratio of 1.9 ┬▒ 0.6 for the worldwide case notification rate. In some countries, this ratio may reach values as high as 3 [25]. The possibility of under-notification of females [26] and poor quality of sputum samples collected from females [27] have been suggested to explain this. However, smoking, alcohol consumption, drug use, exposure to indoor dusts, sex steroid hormones, and the genetic makeup of the sex chromosomes may render males more susceptible to pulmonary TB than females [25]. The results of our study indicate that different susceptibility to outdoor air pollution, especially SO2, may also contribute to gender inequality in TB.
Given the greater prevalence of smoking in males compared to females in South Korea (47.3% vs. 3.1% in 2010) [28], our observation suggests the presence of synergistic effects between SO2 exposure and smoking, which is a risk factor for TB development [29]. In fact, such a synergistic effect on lung function has been reported in a Chinese population [30]. Impaired respiratory defense mechanisms that clear inhaled pollutants [31,32] and changes in respiratory responses [33] caused by smoking may increase the risk of TB development after inhaling M. tuberculosis. However, we could not prove the presence of synergy between SO2 exposure and smoking on the development of TB because of a lack of information on the smoking status of individual TB patients. This is a limitation of our study.
In conclusion, this study provides evidence of an association between outdoor air pollution and an increased risk of TB. Long-term exposure to ambient SO2 increases the risk of TB in males.





 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





