


INTRODUCTION
Biliary tract cancer (BTC) includes intrahepatic cholangiocarcinoma, extrahepatic cholangiocarcinoma, gallbladder cancer, and ampullary carcinoma. The incidence rates of BTC are high in Asia, Latin America, and eastern European countries, while the rates are relatively low in the United States and some western European countries [1]. Approximately 18,000 patients in Japan and 3,200 patients in the United States have died from this life-threatening disease [2,3]. In Korea, approximately 5,400 new patients have been diagnosed, and approximately 3,800 patients have died from BTC [4]. Although the incidence of extrahepatic cholangiocarcinoma has remained constant, the incidence of intrahepatic cholangiocarcinoma has increased recently [3,5].
Curative resection has been considered the only chance to cure this life-threatening disease. Only 10% of patients present with early stage disease and are considered surgical candidates in Western countries [6]. However, curative resection rates have been reported to be 68.1% in cholangiocarcinoma, 68.7% in gallbladder cancer, and 93.0% in ampullary carcinoma from a Japanese registry [7]. The resection rate for BTC differs greatly between Japan and Western countries, a finding that might affect the prognosis of unresectable BTC. However, even patients who are treated with surgery ultimately experience recurrence. Moreover, many patients are still diagnosed at an advanced stage and are not candidates for surgery. Furthermore, there are many elderly BTC patients whose disease is sometimes considered unresectable because of comorbidities. Thus, chemotherapy is indispensable for the treatment of advanced BTC.
Recently, reports concerning chemotherapy for advanced BTC in the first-line setting have increased, and the first-line chemotherapy treatment has gradually become more sophisticated. Additionally, the prognosis of advanced BTC has improved, and the median overall survival has reached almost 1 year [8,9]. However, only limited studies have been reported regarding second-line chemotherapy, and it has not been demonstrated whether second-line chemotherapy can actually improve the prognosis of advanced BTC.
Despite progress in chemotherapy for advanced BTC, several problems have persisted. No consensus regarding surgical indications has been established. Not only cases involving each biliary site but also unresectable and recurrent cases have often all been included in the same study. Assessing these problems and exploring solutions to improve the quality of future evidence for advanced BTC are necessary. Thus, in this review, we summarize the current status of chemotherapy and problems associated with the treatment of advanced BTC. Additionally, we discuss strategies to improve the treatment of this disease.
FIRST-LINE CHEMOTHERAPY
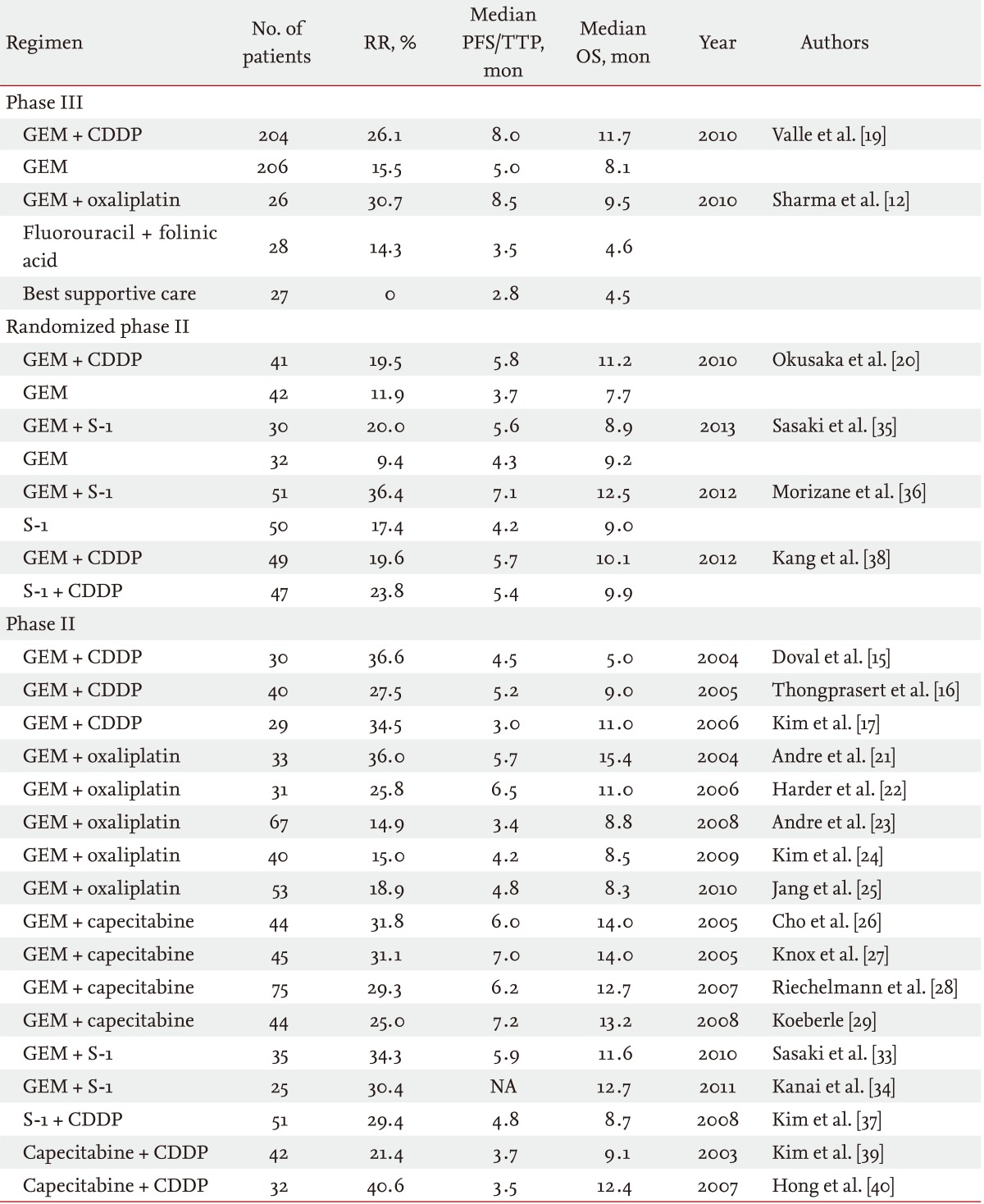
A survival benefit of chemotherapy was suggested in patients with advanced BTC in the first-line setting, based on small randomized controlled studies comparing chemotherapy with best supportive care [10-12]. Subsequently, large retrospective studies were performed, and gemcitabine and platinum were identified as promising agents for the treatment of advanced BTC [13,14]. Several phase II studies of gemcitabine and cisplatin (GC) combination therapy showed a good anti-tumor effect: the median progression-free survival and overall survival were 3.0 to 5.2 months and 5.0 to 11.0 months, respectively (Table 1) [15-17]. Based on these previous analyses, large randomized controlled studies were conducted in the United Kingdom [18,19]. In one randomized phase III study that enrolled 410 patients, the median overall survival with GC combination therapy was significantly improved compared with gemcitabine monotherapy (11.7 months vs. 8.1 months, p < 0.001). The superiority of GC combination therapy to gemcitabine monotherapy was also confirmed by a randomized phase II study (the BT-22 study) conducted in Japan [20]. According to these results, GC combination therapy became the standard of care in patients with advanced BTC in the first-line setting.
Other cytotoxic agents have also been evaluated for first-line chemotherapy in patients with advanced BTC. Gemcitabine and oxaliplatin (GEMOX) has been evaluated widely as an alternative to GC combination therapy [21-25]. The median progression-free survival and overall survival of GEMOX combination therapy were 3.4 to 6.5 months and 8.3 to 15.4 months, respectively. Oral fluoropyrimidines are considered to be the most promising agents, other than platinum compounds. Several previous studies of gemcitabine and capecitabine (GemCap) combination therapy have been conducted [26-29]. The median progression-free survival and overall survival of GemCap combination therapy were 6.0 to 7.2 months and 12.7 to 14.0 months, respectively. According to these promising data, a large randomized phase III study comparing GC combination therapy with GemCap combination therapy was conducted in Canada (ClinicalTrials.gov number, NCT00658593). Unfortunately, this randomized phase III study was stopped in December 2012 due to poor accrual. In Asian countries, particularly Japan, S-1 is widely used for BTC. Several phase II studies using S-1 monotherapy were reported [30-32]. Phase II studies of gemcitabine and S-1 (GS) combination therapy showed a good antitumor effect: the median progression-free survival and overall survival were reported to be 5.9 months and 11.6 to 12.7 months, respectively [33,34]. Regarding GS combination therapy, several regimens (3- and 4-week regimens) were reported from Japan. In the randomized phase II study comparing GS combination therapy (4-week regimen) with gemcitabine monotherapy, GS combination therapy showed a better tumor response and a longer time to progression, but the superiority in overall survival was not sufficient to select this 4-week regimen as a candidate for a phase III study [35]. However, a randomized phase II study that compared GS combination therapy (3-week regimen) with S-1 monotherapy showed the superiority of GS combination therapy to S-1 monotherapy [36]. Based on these results, a large randomized phase III study is now planned to confirm the noninferiority of GS combination therapy using a 3-week regimen of GC combination therapy in Japan. A study of S-1 and cisplatin (SP) combination therapy was also reported from Korea [37]. A randomized phase II study of SP combination therapy versus GC combination therapy showed that both regimens had comparable efficacy with a favorable safety profile as first-line chemotherapy [38]. To confirm the efficacy of SP combination therapy, a phase III study is required. Capecitabine and cisplatin (CP) combination therapy was also evaluated in Korea, and this combination also demonstrated a promising antitumor effect in patients with advanced BTC [39,40]. CP combination therapy also needs further evaluation to confirm its efficacy for advanced BTC. Regarding irinotecan and taxanes, these drugs have only shown a modest antitumor effect in the first-line setting. Thus, they are not actively being evaluated for first-line chemotherapy [41-44].
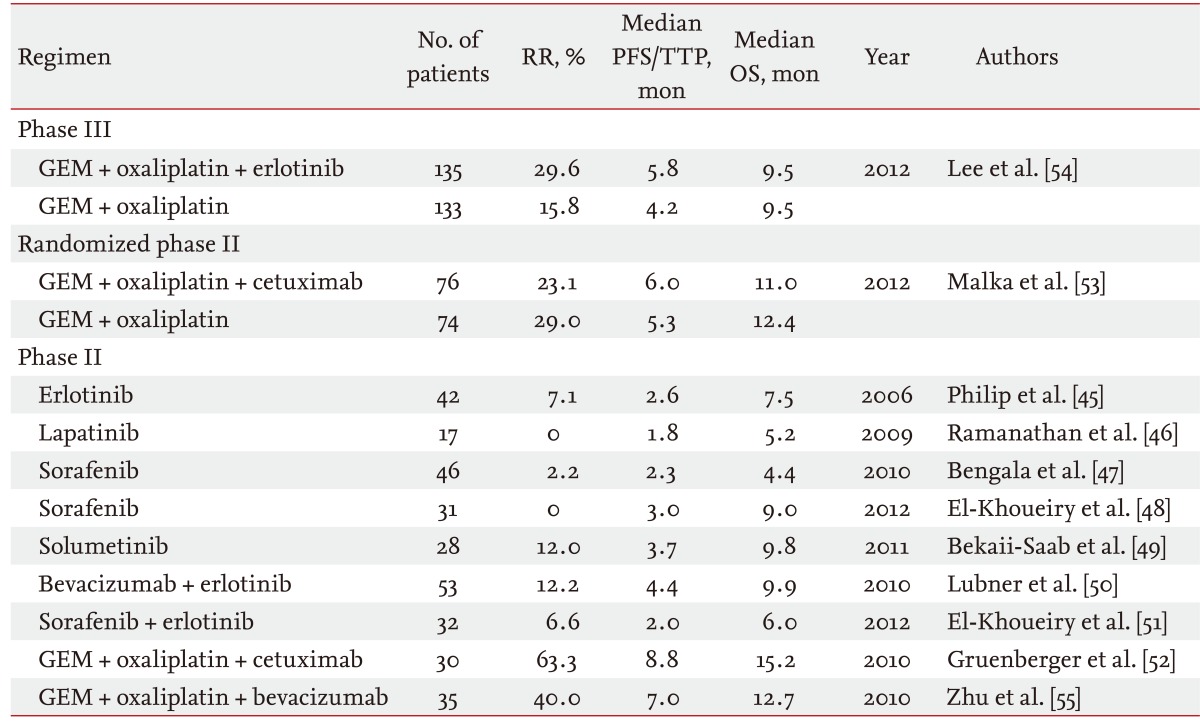
Recently, several prospective studies using molecular targeted agents for the treatment of advanced BTC have been reported (Table 2). Monotherapy using erlotinib, lapatinib, sorafenib, and selumetinib were evaluated; however, antitumor effects using these agents were extremely limited [45-49]. Combination therapy using bevacizumab and erlotinib only showed modest efficacy, with a median overall survival of 9.9 months [50]. Combination therapy using sorafenib and erlotinib also showed limited efficacy [51].
Thus, molecular-targeted agents in combination with cytotoxic agents are now the major strategy for development of new treatment regimens in this field. The combination of GEMOX with cetuximab showed an extremely good antitumor effect in a phase II study with a response rate of 53%, a median progression-free survival of 8.8 months, and a median overall survival of 15.2 months [52]. However, this combination therapy did not show significant superiority versus GEMOX alone in a phase III study, the BINGO trial [53]. Combination therapy of GEMOX with or without erlotinib was also assessed in a phase III setting, although the primary endpoint of progression-free survival was not significantly improved by adding erlotinib to GEMOX [54]. Combination therapy of GEMOX with bevacizumab showed a good antitumor effect in a phase II study, with a tumor response of 40%, a median progression-free survival of 7 months, and a median overall survival of 12.7 months [55]. A phase III study is needed to confirm the efficacy of bevacizumab.
Many prospective studies of first-line chemotherapy are ongoing for the treatment of advanced BTC. Randomized studies of chemotherapy, including phase II and phase III studies, are summarized in Table 3. Additionally, many prospective phase I or II studies, which are not listed in Table 3, are ongoing in many countries.
SECOND-LINE CHEMOTHERAPY
Few data regarding second-line chemotherapy are available for advanced BTC. No clinical study comparing chemotherapy with best supportive care exists. Moreover, the prognoses of patients treated with GC combination therapy in the ABC-02 and BT-22 studies were about the same, although the induction rates of second-line chemotherapy between these two studies were extremely different [19,20]. In the ABC-02 study, only 17.6% of the patients were treated with 5-fluorouracil-based chemotherapy. Conversely, 73.1% of the patients were treated primarily with S-1 in the BT-22 study. Thus, there was no evidence regarding whether second-line chemotherapy actually prolonged the prognosis in advanced BTC.
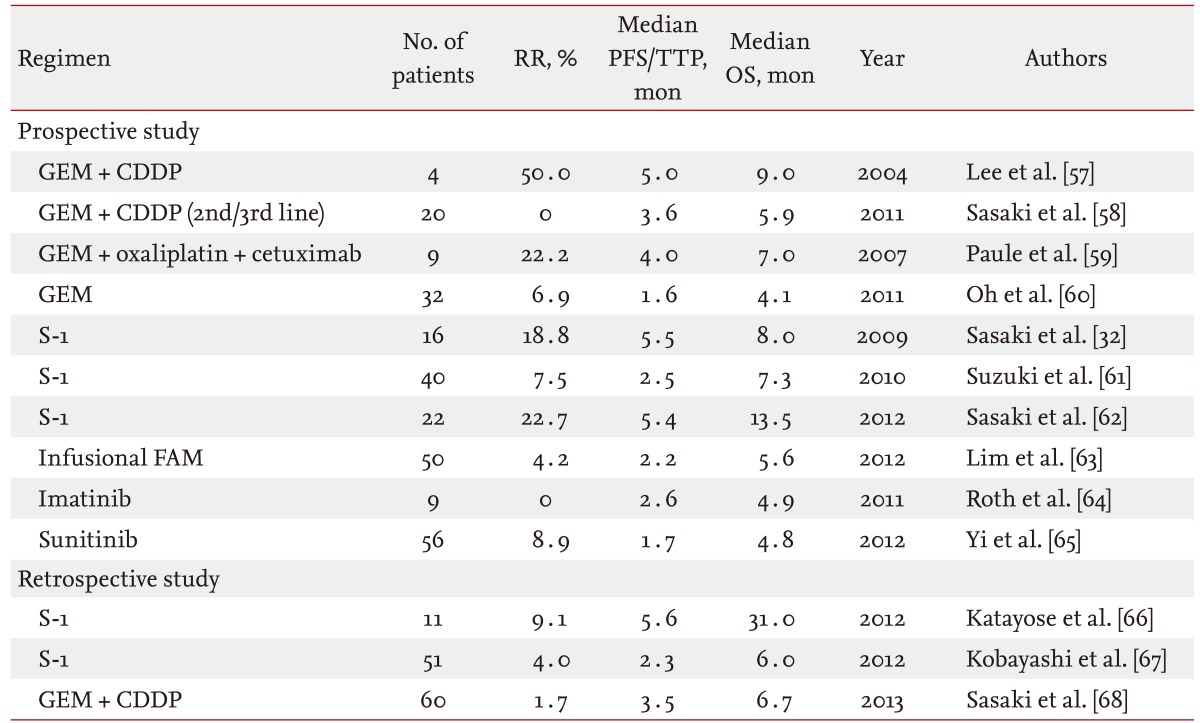
Based on a large retrospective study reported from Canada that enrolled 378 patients, only 96 patients (25%) received second-line chemotherapy [56]. In that study, many treatment regimens were evaluated together. Additionally, the objective response rate and disease control rate were 9% and 43%, respectively. The median progression-free survival and overall survival from the beginning of second-line chemotherapy were 2.8 and 7.5 months, respectively. Doublet chemotherapy and good performance status were extracted as factors associated with a better disease control rate and longer progression-free survival with second-line chemotherapy. Only a few phase II or retrospective studies of some specific regimens have been reported for advanced BTC (Table 4) [32,57-68]. Additionally, a limited number of patients were enrolled in each study, and no comparative study has been reported in the second-line setting. Further evaluation is needed to establish a standard second-line chemotherapy.
PROBLEMS ASSOCIATED WITH CHEMOTHERAPY FOR ADVANCED BTC
Indication criteria for surgery
Indication criteria for surgery have not yet been defined for BTC. It may be difficult to unify the indication criteria of surgery because BTC sometimes needs extended surgery, such as hepatopancreatoduodenectomy, a highly sophisticated surgical technique. Resection rates were significantly different between Western countries and Japan [6,7]. Differences in surgical indication may lead to discrepancies in patient populations, particularly for locally advanced cases. Thus, it is necessary to create some criteria, such as the National Comprehensive Cancer Network guidelines for pancreatic cancer, criteria for resectable, borderline resectable, and unresectable disease [69]. Otherwise, it might be better to use only the data of metastatic patients in a comparative study. Moreover, the reason for unresectable disease should be indicated, in particular, whether it was caused purely by tumor factors. Factors such as patient characteristics are sometimes the cause of unresectable disease, because BTC patients are sometimes elderly and have several comorbidities.
Heterogeneity of the patient population
The patient BTC population is heterogeneous. Because the incidence of BTC is low, both unresectable and recurrent cases are often enrolled in the same study. Moreover, all involved biliary sites are typically analyzed together. However, the treatment outcomes of these subpopulations are considered to differ. In fact, the median overall survivals of unresectable and recurrent patients who were treated using GC combination therapy in the BT-22 study were 9.4 and 16.1 months, respectively [20]. Furthermore, not only the antitumor effect but also the toxicity might differ between unresectable and recurrent cases, based on a pooled analysis of GS combination therapy [70]. Thus, unresectable and recurrent cases should be enrolled in different studies. Recently, adjuvant chemotherapy has been performed widely, and recurrent patients with no prior chemotherapy have decreased spontaneously.
Treatment outcomes according by biliary site were considered to be different. The prognosis of gallbladder cancer was poorer than that of other BTCs [14]. BTCs are a heterogeneous group of diseases not only anatomically but also biologically. BTCs are also a genetically diverse collection of cancers [71]. Further evaluation is needed to identify the differences in each biliary site from both basic and clinical perspectives.
Analysis of tumor volume
Tumor volume was not assessed in most previous studies of advanced BTC. Tumor volume or tumor size is usually a prognostic factor in many other cancers. However, it is generally not discussed in the field of BTC. The patient population in BTC is usually heterogeneous. Thus, a large unresectable gallbladder cancer and a small recurrent liver metastasis are sometimes evaluated in the same patient population. Thus, we believe information regarding tumor volume should be presented together with patient characteristics. We usually use "baseline sum of the longest diameter (BSLD)" as the tumor volume parameter because BSLD is usually measured when the tumor response is judged by the Response Evaluation Criteria in Solid Tumors (RECIST) criteria. Based on our previous analysis using RECIST version 1.0, BSLD was extracted as a prognostic factor for the treatment of GS combination therapy in patients with advanced BTC [72]. Further examination is needed using a large cohort and the new RECIST criteria version 1.1.
Biliary drainage
Biliary drainage is extremely important for safe delivery of chemotherapy. The quality of biliary drainage might also affect the prognosis of advanced BTC. However, few studies provide detailed information regarding biliary drainage during the study treatment. Information concerning how many patients suspended or postponed treatment because of biliary complications is also indispensable. Thus, detailed biliary drainage information should be reported in future studies.
CONCLUSIONS
In the current review, we discussed the current knowledge and problems of chemotherapy for advanced BTC. The evidence for chemotherapy in advanced BTC has increased over the present decade, and the prognosis of patients with advanced BTC has improved. However, treatment regimens are not fully developed compared with other major cancers, such as those for lung cancer and colorectal cancer. Several serious problems identified in the present review remain unsolved. These problems should be addressed immediately before a large amount of evidence is accumulated in the next decade. If the incidence of BTC is too low to overcome these problems, a multinational collaboration should be considered. Global collaboration is essential for the future development of chemotherapy in the field of BTC.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





