


To the Editor,
Although spontaneous coronary artery dissection (SCAD) is well known clinically, the diagnosis of SCAD is occasionally difficult using only conventional coronary angiography (CAG) without additional imaging tools such as intravascular ultrasound (IVUS) or cardiac computed tomography (CCT).
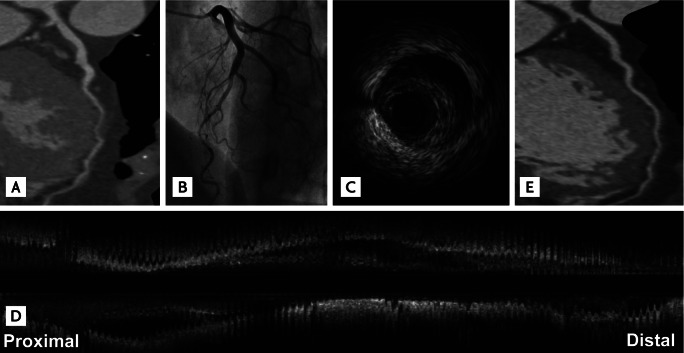
A 55-year-old woman presented to the emergency department with resting anterior chest pain after emotional stress. She had a 7-year history of hypertension. Electrocardiography and transthoracic echocardiography results were unremarkable, and CCT was performed to evaluate the cause of the chest pain. This revealed severe luminal narrowing in the middle part of the left anterior descending coronary artery (LAD) (Fig. 1A). CAG showed 60% stenosis of the middle to distal LAD (Fig. 1B). IVUS to evaluate the lesion revealed coronary artery dissection and a hematoma in the middle LAD, from the 2nd diagonal to the 4th septal branch (Fig. 1C and 1D). As there was no coronary flow limitation and the symptoms stabilized, the patient was managed medically without additional procedures. The 3-month follow-up CCT showed resolution of the compressed luminal narrowing (Fig. 1E).
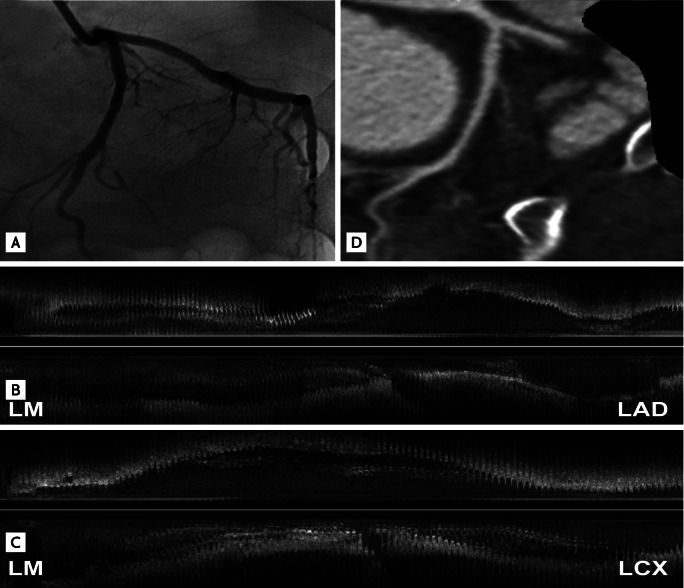
A 70-year-old man presented to the emergency department with sudden-onset severe resting chest pain for 30 minutes. Electrocardiography showed ST segment elevation in leads I and aVL. Emergency CAG revealed mild stenosis in the proximal LAD and left circumflex coronary artery (LCX) (Fig. 2A). The ST-segment elevation resolved spontaneously. IVUS revealed coronary artery dissection and a hematoma from the left main (LM) to the proximal LAD and proximal LCX (Fig. 2B and 2C). The patient was treated medically due to stabilized symptom. One week later, CCT revealed a minimal residual hematoma in the left main bifurcation area (Fig. 2D).
SCAD is a rare cause of acute coronary syndrome. The clinical presentation can range from angina to ST segment elevation myocardial infarction, ventricular fibrillation, and sudden death [1]. SCAD is a hematoma or thrombus in a false lumen, usually in the outer third layer of the coronary artery wall; this compresses the true lumen and leads to coronary ischemia [2]. SCAD should be considered in patients, especially women in the peripartum period and those using oral contraceptives, who complain of chest pain and have atherosclerosis or cardiovascular risk factors, or vascular disease. Other risk factors are connective tissue disorders, cocaine use, exercise, and medications such as 5-fluorouracil, cyclosporine, and fenfluramine.
The etiology and pathophysiology of SCAD are poorly understood [3]. The optimal treatment strategy for SCAD remains undetermined, and treatment varies according to the type and severity of presentation [4]. Treatment options include percutaneous coronary intervention, coronary artery bypass grafting, and conservative medical management such as a ╬▓-blocker to reduce the vascular shear forces and antiplatelet therapy to reduce thrombus formation. The choice is based on the patient's hemodynamic status, coronary artery flow, dissection location, number of involved vessels, and other clinical situations.
The diagnosis of SCAD is made principally based on the appearance of a radiolucent intimal flap or slow clearance of contrast from the false lumen on CAG. When an intimal tear is absent, the medial hematoma can appear as a narrowed or occluded vessel on CAG. The true incidence of SCAD can be underestimated when diagnosed using CAG alone [5]. Imaging tools such as CCT and IVUS can support the diagnosis of SCAD. IVUS can distinguish atherosclerotic stenosis and spasm from hematoma or dissection, and can identify the length of the hematoma or location of the dissection. In addition, IVUS can be used during percutaneous coronary intervention for SCAD. IVUS can facilitate the placement of the angioplasty guidewire within the true lumen; assist in determining stent size, length, and optimal deployment; and ensure obliteration of the false lumen and flow within it, or adequate compression of the intramural hematoma [5]. CCT is an ideal noninvasive imaging technique for delineating intramural hematomas and assessing luminal narrowing. Furthermore, follow-up of SCAD without invasive diagnostic CAG is an important benefit of CCT, as in our cases. To make the diagnosis, a clinical suspicion of SCAD is important when it is difficult to explain the pathogenesis of a stenotic lesion, especially in young patients with no conventional risk factors.
In conclusion, SCAD is an unusual cause of acute coronary syndrome and is difficult to diagnose. Therefore, a clinical suspicion of SCAD and the use of additional imaging tools such as IVUS and CCT are vital. In the presented cases, SCAD was diagnosed successfully using IVUS and followed up using CCT.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





