


INTRODUCTION
Constipation is a digestive symptom that is frequently seen in clinical practice. Its prevalence has been reported to be 2% to 20%, depending on the geographical region [1-3]. Few studies on the prevalence of constipation have been conducted in Korea. A prevalence of 16.5% was reported in one Korean epidemiological study [4]. Constipation may occur because of organic diseases such as endocrine, metabolic or neurological conditions, or colon cancer. However, because most of them appear as functional constipation without an explanatory cause, their management is problematic. In Korea, despite the rapid development of medical science, systematic studies on constipation have been conducted only rarely. Meanwhile, guidelines on the diagnosis [5] and treatment [6] of functional gastrointestinal disorders, including constipation, have recently been proposed by The Korean Society of Neurogastroenterology and Motility (KSNM). Despite the limited data regarding constipation in Korea, these guidelines have been established under the assumption that the results of foreign studies can be applied to the domestic situation, because the difference in the response to drugs among patients of different ethnic backgrounds is insignificant. Furthermore, to overcome limitations, the guidelines refer to data from other Asian countries with a similar epidemiological distribution to that of Korea. To produce guidelines based on a review of domestic and international studies, a consensus among experts was reached using the Delphi method. In addition, a survey via e-mail among doctors in primary and secondary medical institutions was conducted in which the guidelines will be used most frequently, followed by development of clinical treatment guidelines. Therefore, these guidelines are expected to reflect the current situation regarding treatment of constipation in Korea. In this paper, practical constipation treatment methods that are in current use in Korea will be reviewed with reference to these guidelines [6].
DEFINITION OF CONSTIPATION
To establish proper management, identification of the symptoms and an accurate diagnosis are important. It seems that there is no marked difference in the definition used in Korea and that in other countries [4]. Constipation that is perceived by patients is very comprehensive. It includes various features such as propulsive force during defecation, sense of insufficient defecation, hard stools, a sense of barriers to defecation, longer stay in the bathroom, and decreased frequency of defecation [2,3]. Like other countries, the Korean definition of constipation has been established according to the ROME III criteria proposed in 2006 [7]. In these criteria, functional constipation, excepting that caused by organic factors, is defined as including two or more of the following: 1) straining during at least 25% of defecations; 2) lumpy or hard stools in at least 25% of defecations; 3) sensation of incomplete evacuation for at least 25% of defecations; 4) sensation of anorectal obstruction/blockage for at least 25% of defecations; 5) manual maneuvers to facilitate at least 25% of defecations (e.g., digital evacuation, support of the pelvic floor); and 6) fewer than three defecations per week.
ASSESSMENT BEFORE TREATMENT
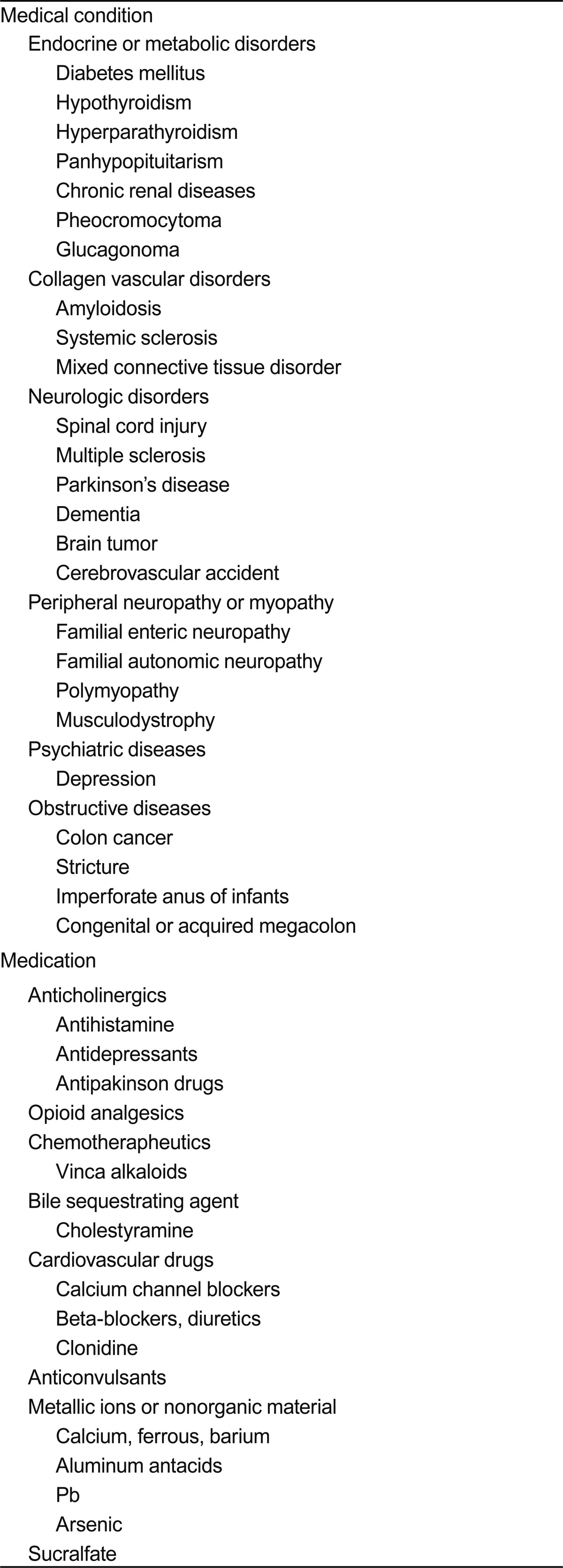
Careful procedures are necessary to exclude secondary constipation. Subjective symptoms can be identified by detailed medical history taking. When patients visit the hospital due to the sudden occurrence of melena, abdominal pain, abdominal distension, and fecal incontinence, an interview appropriate to each situation, including concurrent diseases and current medication, is required. In general, when constipation is associated with identifiable causative factors or systemic diseases, this is called secondary constipation. In particular, the fact that a variety of drugs can cause constipation should be kept in mind. Diseases and drugs frequently related to constipation in Korea are presented in Table 1 [8].
Secondary constipation caused by organic diseases of the colon, rectum, and anus such as colon cancer, stricture, rectocele, and anal fissure is sometimes called organic constipation. In this case, constipation can be cured by treatment of the causative diseases. Other organic forms of constipation are caused by imperforate anus in infants, congenital or acquired megacolon, mucosal prolapse syndrome, and solitary rectal ulcer syndrome.
If secondary constipation with known causative factors is excluded, patients are diagnosed with idiopathic or primary constipation. Idiopathic constipation is classified into normal transit, slow transit, and outlet-obstruction-type constipation. Some patients may present with a combination of these subtypes.
Patients with normal-transit constipation frequently complain of infrequent defecation without delayed colon transit, and tend to be unresponsive to laxatives and fiber supplements [9]. These patients may show increased psychosocial distress and misperceive bowel frequency [9,10].
Slow-transit constipation, also called colonic inertia, is usually associated with dysfunction in the enteric plexus or interstitial cells of Cajal, which are the pacemaker cells of gastrointestinal smooth muscle [11]. The typical finding is delayed passage of radiopaque markers through the proximal colon. This is again divided into delayed colonic transit and motility disorder of the colon due to the diffuse whole gastrointestinal tract.
Outlet-obstruction-type constipation is called anismus, defecation disorder, or pelvic floor dyssynergia. In this type, failure in synergic movements among pelvic floor muscles such as puborectalis, external sphincter, and anal internal sphincter muscles causes inadequate defecation [12]. If outlet-obstructive type constipation is suspected, anorectal manometry and defecography may facilitate differentiation of pelvic floor dyssynergia, rectal intussusception, and rectal prolapse.
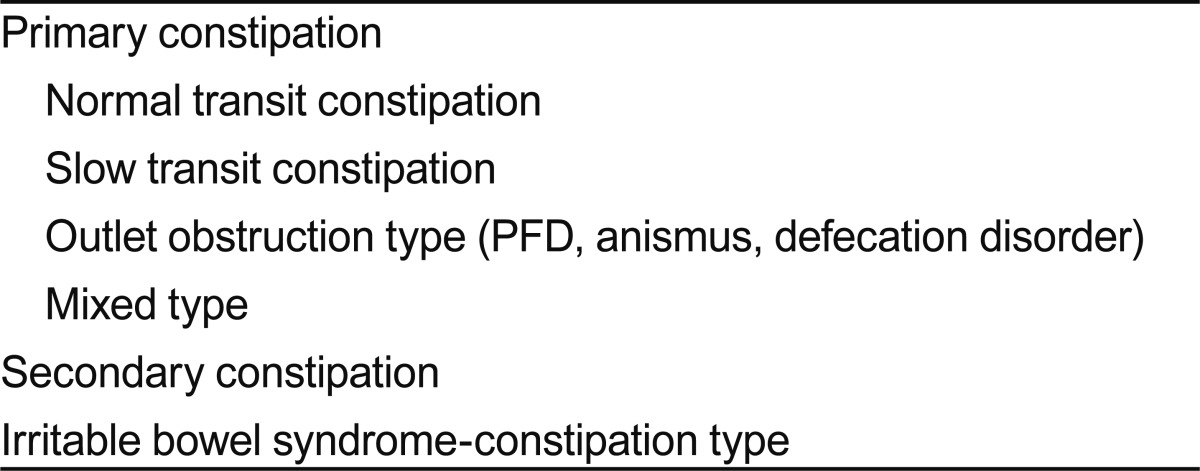
Irritable bowel syndrome of constipation type or constipation period in mixed type may be another cause of constipation. The classification of constipation according to pathogenesis is summarized in Table 2.
Together with other physical examinations, digital rectal examination is essential. It is important because it is a basic method of identifying organic factors such as rectal cancer, and because it can identify constipation with obstructive defecation by assessing the functions of pelvic floor muscles and internal and external anal sphincter via attempted defecation.
In cases of no response to experiential constipation treatment or patients with warning symptoms such as melena and weight loss, colonoscopy or barium enema should be conducted to exclude colon cancer and other organic diseases.
PRACTICAL TREATMENT
As mentioned above, the removal of causative factors is critical to the treatment of secondary constipation, which is beyond the scope of this review. Instead, we mainly discuss the treatment of primary constipation.
Dietary control
Dietary control is the most fundamental constipation treatment method. First of all, patients with constipation should have an appropriate water and fiber intake [8]. Although dietary fiber itself has a minimal effect on constipation treatment, it is fermented by normal flora in the colon and induces its proliferation, causing increased stool volume. Dietary control increases defecation frequency and the amount of stool by softening the stools and increasing their volume by combining with water and ions in the colon, leading to improvement of constipation. Usually, a daily fiber intake of 15 to 25 g per day is recommended with sufficient water (1.5 to 2 L) [13]. Dietary fiber is abundant in grains, fruits, and vegetables. If a large amount of fiber is consumed in a short time, complications such as abdominal distension, belching, and diarrhea may occur. In Korea, it has been reported that dietary fiber supplementation reduces symptoms of constipation without side effects and shortens colonic transit time [14-17]. However, Korean studies have been conducted on a small scale and over a short time, therefore, a further large-scale, long-term randomized controlled study is required. Korean clinicians generally agree that the intake of dietary fiber increases the amount of stool and reduces colonic transit time [6]. Therefore, although the effect of dietary fiber on the treatment of constipation is minimal, it could be used as an early treatment because it has the advantages of easy implementation, no adverse effects, and a low cost.
Changes in lifestyle
It is important for patients to be in the habit of going immediately to the bathroom for defecation when they want to have a bowel movement. The continuous holding of stools contributes to the vicious cycle of constipation by inhibiting neuromuscular reflex and decreasing sensation [13]. For defecation posture, patients who are unable to sit with their back straight are recommended to adopt the squat position with both legs lifting to the abdomen, or the left decubitus position.
Regular exercise such as walking eases defecation by facilitating colonic motility, but evidence is not insufficient. Physical activities including exercise are known to improve the symptoms of colonic motility in some patients [18-20], but results vary depending among individual patients and according to exercise intensity [21]. In Korea, although there has to-date been no report that exercise improves constipation, short-term, small-scale studies have reported that abdominal massage reduces the symptoms of constipation [22,23]. Domestic clinicians generally agree that exercise improves the symptoms of constipation [6]. Therefore, although the correlation of exercise with constipation is unclear in adult patients, exercise is likely to improve the symptoms of constipation in elderly individuals.
Drugs
If no response to the aforementioned methods is observed, drug treatment should be considered. Drugs used for the treatment of constipation are classified as bulk-forming, osmotic, stimulant, and other laxatives, according to their mechanism of action [8].
Bulk-forming laxatives are generally considered as a first-line drug. They are not absorbed through the small intestine, and are not degraded by bacteria in the colon. Thus, they can contain water, which in turn increases stool volume in the intestine and the amount of defecation by increasing the level of water in the stool. They are useful for patients who have a sufficient intake of dietary fiber. Brown rice, bran, plant seeds, seaweed, agar, karaya, methylcellulose, and polycarbophil are examples of these agents. Commercially available drugs in Korea include Mutacil®, Agio®, and Sylcon®. However, if these drugs are used in patients with colonic stricture or obstruction, obstructive symptoms may worsen due to increased stool volume. In general, Korean clinicians agree that bulk-forming laxatives are effective in the treatment of constipation [6], although no long-term study is available.
Osmotic laxatives are not absorbed from the colon. They facilitate defecation by softening stools via an increase in water inside the colon. They are classified into salt and hyperosmolar laxatives. Salt laxatives include various Mg salts and phosphate. Mg ions are not absorbed in the intestine; therefore, the gastrointestinal pressure increases due to retention of water. Thus, Mg ions act as a laxative. However, overdose may cause hypermagnesemia; therefore, Mg ions should be administered carefully to patients with renal failure and to children. Although no study of the effect of Mg laxatives on constipation has been conducted in Korean patients with constipation, Mg laxatives have been widely used in such patients elsewhere [24,25], and Korean clinicians generally agree that these are useful for treatment of constipation [6].
Hyperosmolar laxatives include lactulose, sorbitol, lactitol, glycerin, and polyethylene glycol (PEG). These drugs are not absorbed in the intestine and maintain high osmosis in the colon [26-28]. Thus, defecation occurs in a liquid form due to a lack of absorption of water into the body. Korean clinicians generally agree that administration of PEG and various nonabsorbable polysaccharides is effective for treatment of constipation [6]. Hyperosmolar laxatives are likely to be effective drugs that can be safely administered to patients over a long period.
Stimulant laxatives are used if no response to the aforementioned drugs is observed. Although their exact mechanism of action has not been established, they are known to facilitate colonic motility by inhibiting absorption of water and electrolytes and accumulating water and electrolytes [29-32]. Commonly used stimulant laxatives include anthraquinone drugs (e.g., aloe, senna, or cascara) and polyphenol drugs (e.g., bisacodyl or phenolphthalein). Although there is some disagreement among researchers, short-term use of these drugs for several months is generally recommended [13]. In the case of long-term use, loss of water and electrolytes, secondary hyperaldosteronism, steatorrhea, and protein-losing enteropathy may occur. These drugs are abused without prescription in Korea; therefore, they should be prescribed with caution. Although no study of the effect of stimulant laxatives on constipation has been conducted in Korea, they have been used in some patients [6]. In addition, Korean clinicians generally agree that stimulant laxatives are effective in some constipation patients.
Other laxatives include surfactant laxatives and prokinetics. Surfactant laxatives include docusate, castor oil, mineral oil, and dehydrocholic acid. Although they seem to have a stool-softening effect, their effects on chronic constipation are varied [33-37]. No study of the effect of surfactant laxatives on constipation has been conducted in Korea, but they have been widely used. Korean clinicians generally agree that surfactant laxatives are effective in the treatment of constipation [6].
Representative prokinetic drugs for constipation include 5-HT4 receptor agonists such as cisapride, tegaserod, and prucalopride [38-41]. They mediate intestinal peristalsis via 5-HT4 receptors, and stimulate secretion into the intestinal tract. One Korean study reported that cisapride was effective in constipation [42]. Although it is controversial, most of these drugs are not commercially available due to cardiovascular side effects [43]. Even if they are used, it is difficult to achieve efficacy with prokinetics alone in actual clinical practice. In Korea, 5-HT4 receptor agonists have not been available since tegaserod was withdrawn in 2007. New 5-HT4 receptor agonists such as prucalopride, renzapride, and other enterokinetics that are safe and have few side effects have been developed and introduced into clinical practice in Western countries, and are expected to be widely used in Korea in the near future. Korean clinicians generally agree that 5-HT4 receptor agonists are effective in the treatment of constipation [6].
In the case of a lack of response to the aforementioned drugs, suppositories or enema therapy using saline, sodium phosphate, glycerin, and sorbitol may be considered. Types of laxatives according to mechanism of action and typical drugs commercially available in Korea are summarized in Table 3.
Behavioral therapy
If outlet-obstructive type constipation is suspected, it should be diagnosed through an appropriate evaluation such as anorectal manometry [5]. Subsequently, biofeedback therapy leads to improvement of symptoms in about 70% of cases [44-48]. Biofeedback therapy is an educational strategy that recognizes body responses using electrical or mechanical devices [49]. That is, in chronic constipation patients, biofeedback therapy trains the patients to relax the pelvic floor striated muscle during defecation, and to recognize rectal distension caused even by a small amount of stool and to increase abdominal pressure effectively. Biofeedback therapy has been conducted on constipation patients in Korea. Several Korean studies have reported that biofeedback therapy was effective in 70% to 80% of patients with constipation and pelvic floor dysfunction [50-53], and that its efficacy persisted for than 1 year [50]. Korean clinicians generally agree that biofeedback therapy is effective in the treatment of patients with constipation caused by pelvic floor dysfunction [6].
Surgical treatment
Sacral nerve stimulation (SNS) increases the frequency of defecation and improves constipation symptoms by electrically stimulating the spine and sacral nerve root [54]. The outcomes of this treatment vary [55-58]. Two studies of SNS have been conducted in patients with constipation in Korea, and good treatment outcomes have been reported in patients with slow-transit constipation and impaired rectal sensation [52,59]. Although it is not commonly performed, Korean clinicians agree that SNS is effective in the treatment of constipation [6].
In the case of incurable slow-transit constipation that does not respond to medical treatment, colorectal surgery may be considered [60]. A Korean retrospective study reported relatively high patient satisfaction [61-63]. Korean clinicians generally agree that colorectal surgery is effective in the treatment of some patients with incurable slow-transit constipation [6].
CONCLUSIONS
As described above, there are no marked differences in the treatment of constipation between Korea and other countries. However, the number of comprehensive studies on constipation, such as epidemiology or treatment, is currently insufficient. Thus, the development of treatment guidelines specific for Korean patients, that take into consideration ethnicity and regional characteristics, is required. To this end, the KSNM recently proposed domestic guidelines for the diagnosis and treatment of constipation, which will significantly assist clinicians who treat patients with constipation. The constipation study group of the KSNM has been conducting a large clinical cohort study that has comprehensively investigated constipation, including its perception by the Korean population, and its prevalence and treatment, via a nationwide survey.
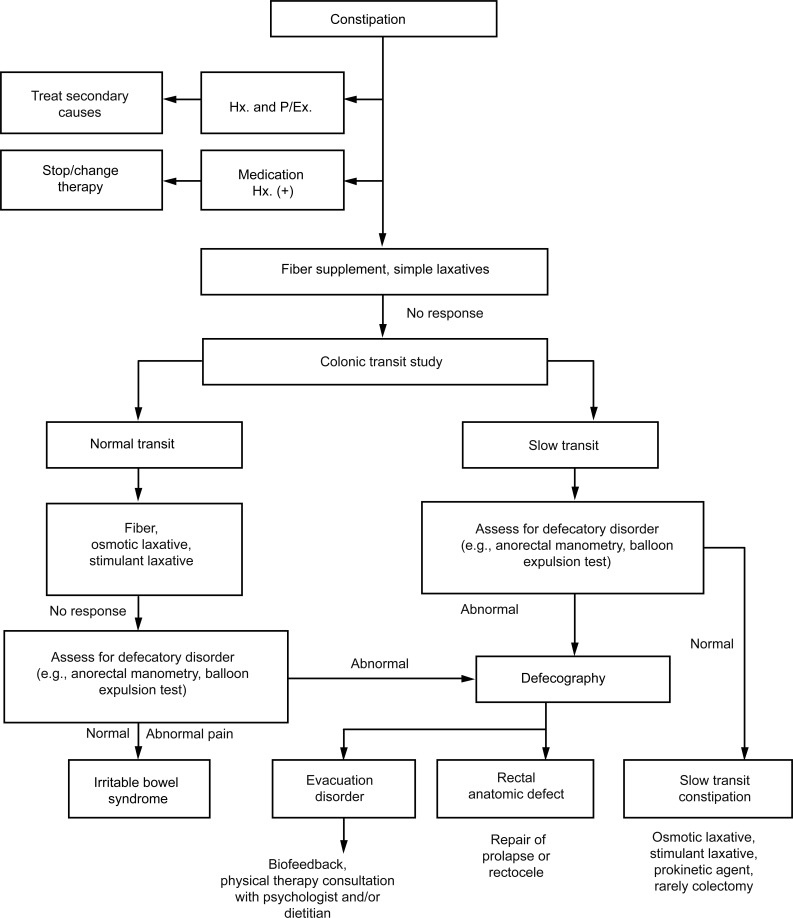
In spite of insufficient data, the practical management algorithm most commonly accepted by Korean clinicians is presented in the Fig. 1. With the interest of clinicians and the efforts of expert groups, the development of guidelines for the treatment of constipation that reflect the domestic situation in Korea is expected to contribute to improvement of the quality of life of patients with constipation.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





