


INTRODUCTION
Kidney transplantation is the most effective treatment for patients with end-stage renal disease (ESRD). However, the incidence of ESRD is growing markedly worldwide; hence, the demand for kidneys exceeds the available supply. This shortage is leading to a progressive increase in the number of patients on waiting lists for transplantation [1].
The trends in donor type vary among countries. For example, in the United States, more than 40% of transplantations come from deceased donors [2,3], whereas in Korea and Japan most transplants use organs from living related donors, and the proportion of deceased donors is low [4,5]. Despite these differences, increasing the supply of donors has become an important issue in most countries.
In Korea, kidneys used for transplantation are predominantly from living donors, and the country has been suffering from a chronic shortage of donors. In 2007, 9,183 patients were diagnosed with ESRD, but only 928 (10.1%) received a kidney transplantation [6]. During the past 40 years, many changes to the donor source have occurred, which may be the result of an effort to overcome the donor shortage in our transplant center. In this study, we reviewed changing trends in donor types and provided detailed information on donor sources. From this analysis, we intend to suggest future directions to help increase the numbers of donors.
METHODS
From March 1969 to December 2008, 1,690 kidney transplantations were performed at Seoul St. Mary's Hospital. We retrospectively reviewed the medical records of the patient population. We collected the baseline characteristics of donors, including age at the time of transplantation, gender, and the relationship between recipient and donor.
To evaluate changing patterns in donor type, we investigated the donor sources during each decade. For convenience, five transplants performed in 1969 were included with those performed the 1970s. We divided the donor population into three groups: living related donor (LRD), living unrelated donor (LUD), and deceased donor (DD). The LRD group was subdivided into parent, sibling, offspring, and distant family groups. The LUD group was subdivided into spouse donors and "others." In addition, we included transplantation cases from outside Korea (overseas transplantation), and we compared this proportion with the caseload in our center.
The results are presented as the mean ┬▒ SD, and p < 0.05 was considered significant. The statistical analysis was performed using the SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Overall number of each donor type
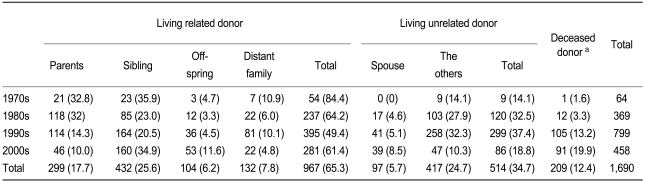
Among 1,690 cases, 1,481 (57.2%) were from LDs and 209 (42.8%) were from DDs. Among 1,481 LD transplants, 967 were from LRDs (65.3%) and 514 were from LUDs (34.7%). Among 967 LRD transplants 432 were from sibling donors (44.7%), 299 from parental donors (30.9%), 104 from offspring (18.8%), and 132 cases (13.7%) from distant family members. Among 514 LUD transplants, 97 (18.8%) were from spouse donors, and 417 (81.2%) were from "other" unrelated donors, such as friends or volunteers (Fig. 1).
Changing pattern of donor age and living donor gender
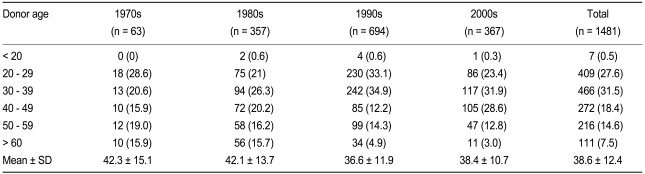
The mean age of LDs was 38.6 ┬▒ 12.4 years in the 2000s decreased from 42.3 years in the 1970s. In contrast, the mean age of kidney recipients has increased gradually. Most donors were from 30 to 39 years of age (31.5%), and donors aged less than 20 years were the smallest group (0.5%). The overall male-to-female ratio of donors was 1:0.73 (823:658). Until 1989, the case numbers of male and female donors were almost equal or slightly female-dominant, with a ratio of 1:1.03 (31:32) in the 1970s and 1:1.11 (169:188) in the 1980s. However, after 1990, male donors exceeded female donors significantly, with ratios of 1:0.59 (434:260) in the 1990s and 1:0.94 (189:178) in the 2000s (Table 1).
Changing pattern of living related donors
During all four decades, the major type of living donor transplantation was from LRDs. During the 1970s, these comprised 84.3% of total transplantations (54/64). The LRD proportion decreased to 64.2% (237/369) in the 1980s, 49.4% (395/799) in the 1990s, and 61.4% (281/458) in the 2000s (Fig. 1). Thus, the proportion of LRD decreased markedly during the follow-up period. Within the LRD group, sibling and parental donors were the two main donor types. Sibling donors were the main donor type during all four decades, whereas the parental donor proportion decreased gradually from 32.8% in the 1970s to 10.0% in the 2000s. Offspring donors stayed at a constant proportion of 5% until the 1990s and then increased to 11.6% after 2000 (Table 2).
Changing pattern of living unrelated donors
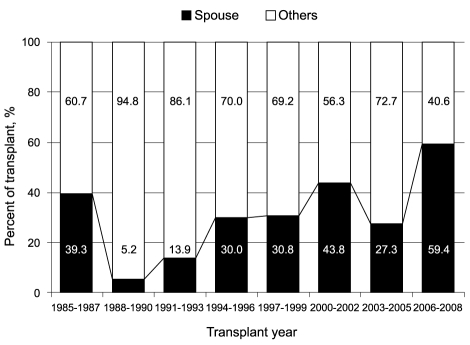
Only 9/94 LUD transplantations (14.1%) occurred during the 1970s. However, the LUD proportion increased from the late 1980s and remained around 20% without much change after 2000. Within the LUD group, the proportion of spouse donors increased remarkably. The first spouse donor transplantation was performed in 1985, and 17 cases were performed during the following 5 years. The proportion was 5.1% (41/799) in the 1990s, increasing to 8.1% (39/458) after 2000 (Table 2). The proportion of first spouse donor transplantation within the LUD group also increased gradually, and spouse donors provided more than half of all LUD transplants after 2006 (Fig. 2).
Changing pattern of deceased donors
The first DD transplantation in our center was performed in 1979. However, this donor type was minimal, and only 13 cases were transplanted until 1989, or only 3.3% of all transplantations during that period. Both the proportions and the case numbers of DD increased gradually to 13.2% (105/799) in the 1990s and 19.9% (91/458) after 2000 (Fig. 1).
Changing pattern of overseas transplantation
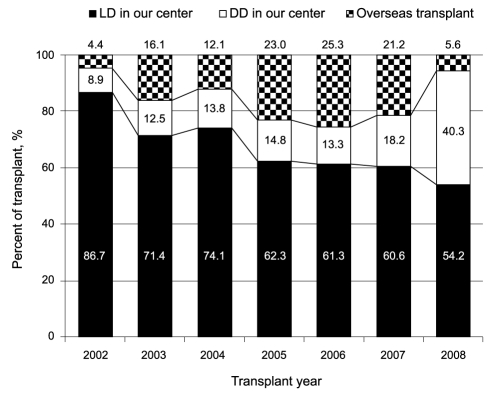
Before 2000, only three patients visited our center after receiving kidney transplantation in a foreign country, and all were from the USA. After 2002, overseas transplantation increased markedly. Thus, 69 patients visited our center after receiving a kidney by "transplant tourism," and the proportion reached 16.7% (69/414) of the caseload seen in our center during the same period. Among these, 66 transplants were performed in China, and three were performed in the Philippines. The number of such foreign transplantations peaked in 2006 (equivalent to 25.3% of all cases seen in our center) and decreased markedly in 2008 (equivalent to 5.6% of all cases seen in our center) (Fig. 3).
DISCUSSION
We reviewed the changing pattern of donor type and clinical characteristics during the past 40 years in our center. The results of our study demonstrate that the proportion of LRDs decreased, whereas the proportions of DDs and spouse donors increased. This finding suggests that the LRD-based donor pattern is changing to a DD and spouse donor base.
The remarkable finding about the LD characteristics is the decreasing donor age and the increasing proportion of male donors. In the 1970s, the proportion of donors older than 50 years reached 34.9% and then decreased gradually to 15.8% in the 2000s. Interestingly, this change coincided with changes in donor type, such as a decrease in the number of parental donors. Thus, the decrease in mean age may have been associated with a change in donor type. After the 1990s, male donors significantly exceeded female donors. The total population numbers of males and females are similar in Korea. However, considering the population aged between 20 and 50 years, which is the group most actively involved in organ donation, males have markedly exceeded females after the 1990s [7]. Hence, the excess number of male donors might result from the recent male dominance in the age group of potential eligible donors.
The most important finding in this study is that the proportion of LRDs decreased. Most renal transplantations in Korea were performed from LRDs, and, in our center, the major proportion of kidney donors was in the LRD group during the study period. This is related to the structure of Korean society, in which familial relations are regarded as very valuable. The reasons for the decreased proportion of LRDs might be multi-factorial. However, we postulate that changes in the social environment are the most important factor. During the past 40 years, Korean society has industrialized rapidly, causing many changes. For example, most Korean families changed to a "nuclear family" model, and the birth rate decreased rapidly. Thus, nearly 50% of families had more than five members in 1980, and this proportion decreased to 28% in 1990 and only 13% in 2000 [7]. The birth rate per family has also decreased significantly, from 4.53 in 1970 to 2.82 in 1980 and 1.07 in 2005 [7]. Therefore, the changes in family structure and low birth rate will gradually reduce the available numbers of sibling donors, who have formed a significant proportion of LRDs. Thus, from our study, we predict that the LRD group might not be a major donor source in the near future.
The LRD subtypes also showed changes, as the numbers of parental donors decreased, but offspring donors increased during the follow-up period. This discrepancy between parental and offspring donors may be related to the changing pattern of ESRD in Korea. For instance, the mean age of patients with ESRD increased markedly and the proportion of elderly patients expanded significantly during the past four decades, according to a report by the ESRD Registry Committee [6]. This change might have been affected by other changes, such as the shift in the main cause of ESRD to diabetes and the increased duration of maintenance dialysis. Obviously, elderly patients with ESRD are less likely to receive a kidney from a parental donor. Also, our center experienced an increase in the mean age of kidney recipients. Hence, it is probable that these changes in the characteristics of patients with ESRD affected the LRD subtype distribution and the mean age of donors.
The LUD group was the second most important source of donor kidneys in our transplant center. During the 1970s, only 9/94 LUD transplants (14%) were performed. The proportion increased in the 1980s (32.5%) and 1990s (37.4%), but decreased to around 20% in the 2000s [8]. This decrease was related to the strict regulation of LUDs in our transplant center. Interestingly, both the proportion and the number of spouse donor cases increased despite the decrease in total LUD cases. The first spouse donor transplantation was performed in 1985, and 17 cases were performed during the subsequent 5 years. The proportion was 5.1% (41/799) in the 1990s and increased to 8.1% (39/458) after 2000. Within the LUD group, the proportion of spouse donors was more than half in recent years, such as 59.4% during 2006 to 2008 (Fig. 2). The reason for this increase in spouse donors might be multifactorial. First, spouse donors are not limited by legal and ethical problems. Second, the graft outcome from a spouse donor is as good as from an LRD [9,10] or other LUDs [11]. Third, in a nuclear family system, it is natural to prefer one's spouse as an organ source to other familial members.
The rate of DD transplantations in our center increased from 3.3% (12 cases) during the 1980s to 20% (91 cases) during the 2000s and it has increased annually since 2000 to reach 40.3% in 2008. This change was related to the establishment of Korean laws defining brain death and the development of public support systems. Previously, DD transplantation was performed without legislation, which raised troublesome social and legal issues. In addition, due to the absence of a nationwide network or data bank to maintain a transplant waiting list, it was not always possible to locate a recipient for an organ from a brain-dead donor [12]. Thanks to the efforts of many transplant physicians and social institutions, a brain death law was established, and the "Korean Network for Organ Sharing" was developed in 2000. Of even greater importance, social attention to organ donation has since increased in Korea. Actually, the proportion of DD was 40.2% of all Korean kidney transplantations in 2008, and it is very similar to that for our center [13]. Hence, we expect that DD transplantation will form the major donor source in the near future in Korea.
Overseas transplantation became an important donor source in Korea after 2000 and reached nearly 20% of all cases in our hospital from 2002 to 2008. The annual number of patients with newly developed ESRD increased by 67% (from 5500 in 2001 to 9183 in 2007). However, the annual number of transplants increased only by 9.4% (from 848 in 2001 to 928 in 2007), and the proportion of transplantations among patients with newly developed ESRD decreased from 15.4% in 2001 to 10.1% in 2007 [6]. This organ shortage drove greater numbers of patients to seek transplantation outside Korea after 2002. However, such transplantations peaked in 2006 and decreased markedly thereafter [14]. Thus, we expect that transplantation in foreign countries will no longer be an important donor source for Korean patients.
In conclusion, the sources of donor kidneys have changed significantly during the past 40 years, along with changes in Korean society. The proportion of LRDs has decreased, whereas the proportions of DD and spouse donors has increased gradually, and they will form the major sources in the future. We expect that this study could be an important reference for other countries to estimate future changes in donor type.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





