


INTRODUCTION
Systolic or diastolic dyssynchrony refers to temporal differences in the peak systolic contraction or active early diastolic relaxation of different myocardial segments. Most previous studies assessing dyssynchrony focused on systolic heart failure with a wide or narrow QRS complex [1]. Recent studies, however, have focused on heart failure patients with a normal ejection fraction (so-called diastolic heart failure). In both heart-failure groups, systolic dyssynchrony was found in 30% to 40% of cases, with diastolic dyssynchrony in about 60% of cases [2]. Intriguingly, the conditions are rarely seen in the same patient. For example, in a recent study of diastolic heart failure, systolic and diastolic dyssynchrony were observed in about 40% of cases, respectively, and were coincident less than 15% of the time [3]. Therefore, these two conditions do not occur in parallel. Furthermore, few studies have examined left ventricular (LV) dyssynchrony in cases of diastolic dysfunction without overt symptoms of heart failure.
Considering the results of the aforementioned studies of diastolic heart failure, we hypothesized that systolic or diastolic dyssynchrony can be detected based on the degree of diastolic impairment in patients with isolated diastolic dysfunction. In the present study, the ratio of the transmitral early peak diastolic velocity to the early diastolic mitral annulus velocity (E/E' ratio) was used to assess the degree of diastolic impairment, and both types of dyssynchrony were quantified using tissue Doppler imaging (TDI) and 2-dimensional speckle tracking imaging (2D-STI).
METHODS
Subjects
Individuals with a preserved LV ejection fraction (LVEF) and no overt symptoms of heart failure according to the Framingham criteria [4] were enrolled in the present study when echocardiographic studies were performed and were found to be appropriate for analysis by TDI and 2D-STI. Subjects with atrial fibrillation or a bundle branch block as shown by electrocardiography were excluded, as were those with a < 50% LVEF or valvular heart disease. Ultimately, 105 subjects (58 males and 47 females) were included. Among the subjects were four cases of hypertension and two cases of diabetes mellitus.
Standard echocardiographic study
Two-dimensional and Doppler echocardiographic examinations were performed using a 3.5-MHz transducer (Vivid 7, Vingmed-General Electric, Horten, Norway). The LVEF was determined in the apical 4- and 2-chamber views using a modified version of Simpson's formula. A preserved LVEF was defined as an ejection fraction Ōēź 50%. The myocardial wall thickness and chamber dimensions were measured in the M-mode; the wall-motion score index was also examined to identify subjects with regional wall motion abnormalities.
As described previously [8], pulsed-wave Doppler echocardiography was performed in the apical 4-chamber view to determine the mitral inflow profile, including the E- and A-wave velocities, E-deceleration time (DT), and E/A ratio. To obtain the peak systolic (Sm) and peak early diastolic mitral annulus velocity (Em), TDI was performed using a 1 mm to 2 mm sample volume on the septal side of the mitral annulus in the apical 4-chamber view.
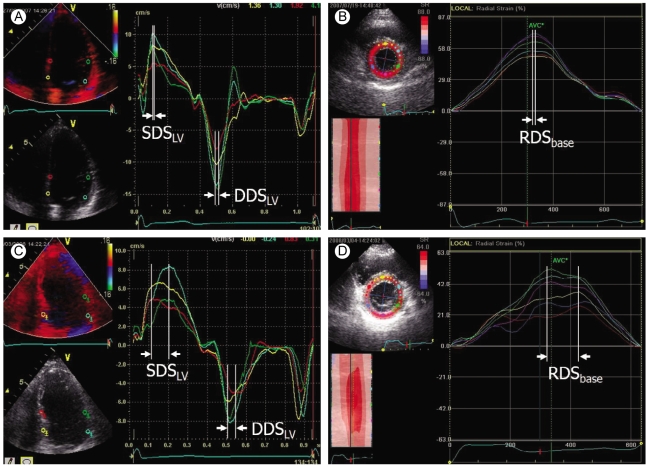
Measurement of systolic and diastolic dyssynchrony using TDI and 2D-STI (Fig. 1)
At least three consecutive beats were stored, and the images were analyzed offline with the aid of a customized software package (EchoPac version 5.1.1, Vingmed-General Electric). To identify LV intraventricular dyssynchrony, the peak myocardial systolic and peak myocardial early diastolic velocities of the tissue Doppler signal were measured using the onset of the QRS complex as a reference point, wherein the basal segments were scanned just above the mitral annulus while the middle segments were scanned at the papillary muscle level. LV intraventricular systolic dyssynchrony (SDSLV) was defined as the difference between the shortest and longest times of the peak myocardial systolic velocity among twelve segments. Likewise, LV intraventricular diastolic dyssynchrony (DDSLV) was defined as the difference between the shortest and longest times of the peak myocardial early diastolic velocity among twelve segments.
At three levels in the apical short-axis view, speckle tracking routine grayscale images were acquired as described previously [9,10]. An end-systolic circular region of interest (ROI) was traced through the endocardial border using a point-and-click technique to adjust the tracking in all six segments. In turn, a larger concentric circle was generated automatically, which had to be adjusted manually near the epicardial border. Shifts in the location of the acoustic markers for each ROI between frames, which represented tissue movement, provided spatial and temporal data for calculating the velocity vectors wherein temporal alterations in the stable speckle patterns were identified as moving farther apart or closer together. A series of regional strain vectors were calculated based on changes in the length/initial length ratio. Myocardial thickening was assigned a positive value, whereas myocardial thinning was assigned a negative value. The software package used automatically created radial strain curves for each segment, which were used to assess radial dyssynchrony. The software package was also used to calculate LV rotation and peak LV torsion using the same grayscale images with a simple change in the analysis mode that allowed frame-by-frame calculation of the rotational angle of the stable speckles. Counterclockwise rotation independent of the LV apex was expressed as a positive value, whereas clockwise rotation was expressed as a negative value.
Radial dyssynchrony was defined as the time difference between the first and last peak values of the radial strain curves at each level (RDSbase, RDSmid, and RDSapex for radial dyssynchrony in the basal, mid, and apical levels in the apical short-axis view, respectively). Peak LV torsion was defined as the difference in degree between the peak apical and basal rotational degrees in the apical short-axis view.
Statistical analysis
Continuous data are presented as the mean ┬▒ standard deviation (SD) unless otherwise stated. Comparisons of the continuous data among the groups were conducted by ANOVA with post-hoc analysis and chi-square tests for comparing categorical data. The relationship between the continuous variables was examined by regression analysis; selection of the most powerful factor was performed using a forward stepwise multivariate analysis (SPSS version 12, SPSS Inc., Chicago, IL, USA). A p value Ōēż 0.05 was used to define a significant result.
RESULTS
Clinical characteristics
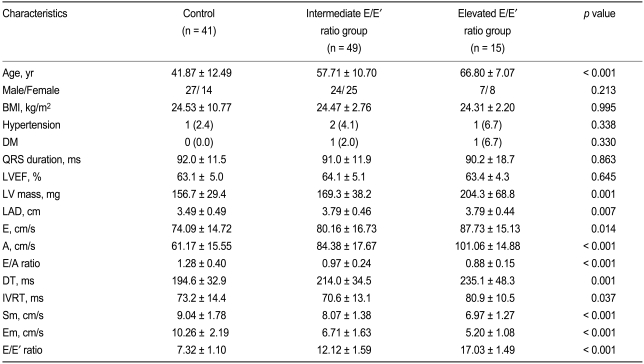
The mean age in the three groups increased according to the degree of increase in the E/E' ratio for the controls compared to that in the elevated E/E' ratio group (p < 0.001, Table 1). However, those subjects with an intermediate or elevated E/E' ratio were similar to the controls in terms of gender distribution, body mass index (BMI), LVEF, and QRS duration.
The LV mass and left atrial dimension (LAD) in the elevated E/E' ratio group were significantly greater than in the controls (p = 0.001 and 0.007, respectively). As shown in Table 1, the mean mitral inflow and annular velocity values differed among the groups.
Analysis of LV interventricular dyssynchrony by TDI
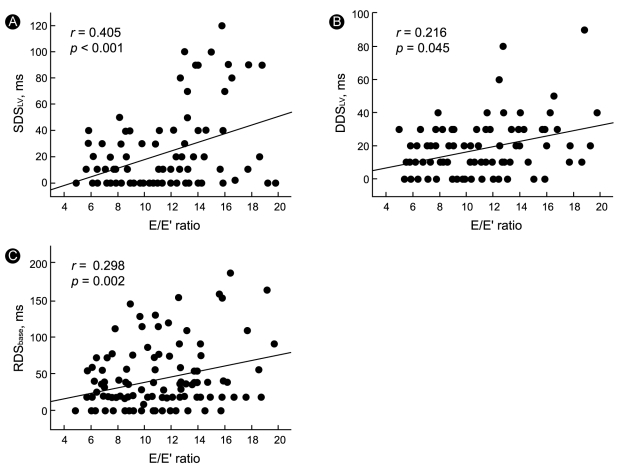
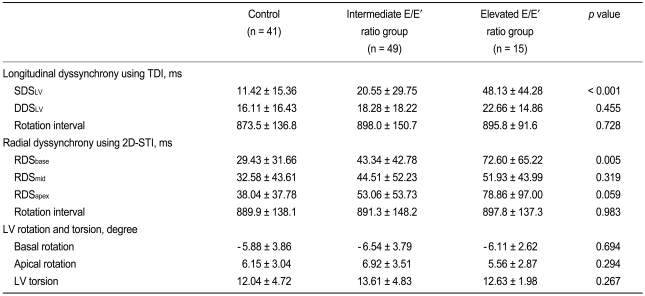
The mean SDSLV in the elevated E/E' ratio group was significantly greater than that in the control group, whereas the mean DDSLV was not significantly different (Table 2). By univariate analysis, significant relationships were identified between the SDSLV and DDSLV and increases in the E/E' ratio (r = 0.405 and p < 0.001 vs. r = 0.216 and p = 0.045, respectively; Fig. 2).
Analysis of LV interventricular dyssynchrony and LV torsion by 2D-STI
The mean RDSbase value in the three groups gradually increased with unchanging significance according to the degree of increase in the E/E' ratio for the control and elevated E/E' ratio groups (p = 0.005), whereas the mean RDSmid and RDSapex values increased with a change in significance (Table 2). Univariate analysis revealed significant relationships between RDSbase and RDSapex and the increase in E/E' (r = 0.298 and p = 0.002 vs. r = 0.196 and p = 0.045, respectively; Fig. 2).
The mean values for the basal and apical rotations did not differ significantly among the three groups, as was the case for LV torsion; no relationship was detected between LV torsion and the E/E' ratio.
Prevalence of dyssynchrony in isolated diastolic dysfunction
Using the cut-off values proposed by Yu et al. [3], for SDSLV (100 ms) and DDSLV (113 ms), four cases of systolic dyssynchrony were identified (6.3%, one in the intermediate E/E' ratio group and three in the elevated E/E' ratio group); none of the subjects had diastolic dyssynchrony or co-existing systolic and diastolic dyssynchrony. Significant radial dyssynchrony was defined as > 130 ms by Suffoletto et al. [9]. According to this criterion, radial dyssynchrony was observed in six cases in the present study (9.4%, two in the intermediate E/E' ratio group and four in the elevated E/E' ratio group).
Adjustment for age
As advanced age can result in various physiologic changes in the myocardium, it is reasonable that the above results should be adjusted for age. After adjustment for age using a stepwise multivariate analysis, SDSLV and DDSLV were found to be significantly related to increases in the E/E' ratio (r = 0.405 and p < 0.001 vs. r = 0.216 and p = 0.045, respectively). RDSbase and RDSapex were also significantly related to increases in the E/E' ratio (r = 0.298 and p = 0.002 vs. r = 0.196 and p = 0.045, respectively). A significant relationship was identified between LV torsion and age (r = 0.210 and p = 0.034) rather than E/E'.
DISCUSSION
The present study may be the first to examine the existence of SDSLV and DDSLV in subjects with isolated diastolic dysfunction but without overt symptoms of heart failure. Systolic dyssynchrony is a relatively common finding in patients with systolic heart failure who have wide QRS complexes [11], and it is also observed in patients with a normal QRS duration [11,12]. Recent studies have focused on heart failure patients with a preserved LVEF, in which wide QRS complexes are rare [1]. Wang et al. [2] reported that systolic dyssynchrony occurred in 30% to 40% of both types of heart failure groups, whereas diastolic dyssynchrony occurred under 60%. Diastolic dyssynchrony appears to be more common than systolic dyssynchrony, and the two are rarely present in the same patient [13]. Furthermore, a combined measurement of longitudinal and radial dyssynchrony was introduced to improve the predictability of cardiac resynchronization therapy (CRT) [10]. In this study, more than one-third of the CRT candidates presented with heterogeneous patterns of positive radial dyssynchrony or positive longitudinal dyssynchrony. Therefore, the assessment of cardiac dyssynchrony requires a multidimensional evaluation, which is why we measured systolic and diastolic dyssynchrony using TDI and radial dyssynchrony using 2D-STI in this study.
In the present study, systolic and radial dyssynchrony were rarely observed, and diastolic dyssynchrony was not observed when the cut-off values determined in previous studies were applied [3,9]. The reason for this may be that the present study was not performed with subjects who presented with diastolic heart failure, only diastolic dysfunction. However, the degree of systolic and diastolic dyssynchrony was found to increase with increases in the E/E' ratio, an indicator of diastolic dysfunction. The E/E' ratio correlates well with the LV filling pressure and pulmonary capillary wedge pressure (PCWP) [14], so it is possible that mechanical dyssynchrony is related to increased myocardial wall tension (stress). The mechanism of mechanical dyssynchrony in diastolic heart failure, in which wide QRS complexes are rarely observed, is unknown, whereas electrical dyssynchrony contributes to mechanical dyssynchrony in systolic heart failure with wide QRS complexes. Moreover, electrical dyssynchrony is not always matched with mechanical dyssynchrony and vice versa [10]. Thus, another pathogenic mechanism may be involved in the manifestation of mechanical dyssynchrony along with electrical dyssynchrony.
Wang et al. [2] reported that medical therapy caused significant shortening of the diastolic intraventricular time delay in patients with diastolic heart failure, in which mechanical dyssynchrony has a reversible component. As a factor in this reversible component, increased wall stress, which causes regional heterogeneity in coronary blood flow and contractile myocardial function, is also suggested. This mechanism is supported by a study using positron emission tomography, which found the presence of abnormal regional myocardial blood flow with respect to the degree of LV hypertrophy [15]. Therefore, the relationship between the degree of systolic and diastolic dyssynchrony and E/E' is not just an incidental finding, but deserves attention, as it may facilitate our understanding of the mechanism of mechanical dyssynchrony in patients with narrow QRS complexes.
Study limitations
The number of subjects was relatively small; a greater number of subjects are needed to produce a more accurate representation of the prevalence of mechanical dyssynchrony in this kind of clinical condition. The E/E' ratio was used to non-invasively estimate the LV filling pressure or PCWP because cardiac catheterization seemed too invasive for use in our subjects, who did not present with overt symptoms of heart failure.
In conclusion, systolic and diastolic dyssynchrony in subjects with isolated diastolic dysfunction but without overt symptoms of heart failure was not as common as in patients with diastolic heart failure. However, the systolic and diastolic intraventricular time delay increased with respect to increases in the E/E' ratio, an indicator of diastolic dysfunction.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





