


INTRODUCTION
Acute myocardial infarction (AMI) is a multi-factorial disease. AMI is often caused by unstable plaque in the epicardial coronary artery, in which inflammatory processes play a central role [1]. In this regard, several circulating pro-inflammatory molecules have been associated with thrombotic cardiovascular events including acute phase proteins, cellular adhesion molecules, and cytokines [2]. Moreover, few articles have explored the predictive value of inflammatory markers on cardiovascular events in cardiovascular disease-free subjects [3,4]. Far fewer studies have considered multiple markers, such as interleukin (IL)-6, tumor necrosis factor-╬▒ (TNF-╬▒), and IL-10 simultaneously. In fact, most studies have focused only on C-reactive protein (CRP) [5]. A recent longitudinal study demonstrated a stronger role for IL-6 in the prediction of congestive heart failure, as compared with CRP [3].
Animal experiments suggest that IL-6 and TNF-╬▒ play important roles in the regulation of acute phase protein synthesis. Acute phase proteins, such as fibrinogen and factor VIII, are established risk factors for atherosclerosis [6]. The plasma cytokine IL-6 plays an important role in mediating inflammation and is a central stimulus for the acute phase response [7].
The effects of inflammatory stimuli are counterbalanced by anti-inflammatory mechanisms, including IL-10, IL-4, high-density lipoproteins (HDL), and vascular endothelial growth factor [8,9]. IL-10 is a centrally operating anti-inflammatory cytokine that plays a crucial role in the regulation of the innate immune system. Studies using IL-10 deficient mice have shown that IL-10 has a protective role in atherosclerosis [10]. Further, it strongly deactivates the inflammatory host response and potently inhibits the production of pro-inflammatory cytokines [11].
The present study was performed to investigate the association between anti- and pro-inflammatory cytokines ratios and AMI.
METHODS
Subjects
The study population was composed of individuals from the eastern part of India of Asian-Indian origin with a history suggestive of AMI. All cases (n = 90) were evaluated using electrocardiographic (ECG) criteria, cardiac enzyme studies, and echocardiographic evaluation (evidence of regional wall motion abnormalities and left ventricular ejection fraction > 50%). All recruited patients were admitted within 12 hours after the first episode of chest pain. Healthy age- and sex-matched controls (n = 90) included subjects without any of the following characteristics: signs of ischemic heart disease, ECG criteria suggestive of acute coronary syndrome, or a past history of cardiovascular disease and diabetes. Samples were obtained from consecutively examined patients except for those with the following exclusion criteria: patients taking known lipid altering medications; use of non-steroidal, anti-inflammatory drugs; and the presence of chronic kidney disease. All patients were admitted to the hospital within 12 hours of the onset of chest pain. Blood samples for cytokine and biochemical analysis were taken at the time of admission. Blood samples were collected by vein puncture into vacuum tubes containing EDTA. Plasma samples were processed and divided into aliquots and stored in cryovials at -700Ōäā until further analysis for cytokines.
The demographic characteristics of patients and control subjects are shown in Table 1. The subjects of the present study were part of a health examination between the Immunotechnology Section (presently Division of Molecular Medicine), Bose Institute Kolkata, and the Department of Cardiology, NRS Medical College and Hospital, Kolkata. Participants between 45 and 65 years of age were recruited between November 2006 and September 2007. The institutional ethics committee approved the study protocol.
Blood biochemistry
Detailed self-reported questionnaires containing information on the history of hypertension, smoking status, and alcohol consumption were collected at baseline and used for analysis. Waist circumferences were also measured according to standard methods. The following parameters were measured using standard methods in our laboratory: glucose, total cholesterol, and HDL cholesterol (HDL-C). Low-density lipoprotein cholesterol (LDL-C) levels were calculated using the Friedewald equation [12] and non-HDL-C levels were calculated as follows: Non-HDL-C = Total cholesterol - HDL-C.
IL-6, TNF-╬▒, and IL-10 levels were measured from frozen stored plasma. Cytokines were measured in duplicate using an enzyme-linked immunosorbance assay kit from Diaclone Research, Besancon, France. These assay kits had a lower limit of detection of 8 pg/mL for TNF-╬▒, 2 pg/mL for IL-6, and 5 pg/mL for IL-10.
Statistical analysis
Results are presented as the means ┬▒ SD and the percentage of the population studied. Student's t tests and Mann-Whitney U tests were used to examine differences between the two groups. For determination of optimal cut-off values and diagnostic performance of these continuous variables, receiver operating characteristic curves analysis was performed. Optimal cut-off points for these risk factors were determined based on the convergence of sensitivity and specificity. Stepwise logistic regression analysis was used to assess the independent adjusted relationship between different variables and AMI with independent variables being those with p Ōēż 0.05 in univariate analysis. All statistical tests were two-sided. A p value < 0.05 was considered to be statistically significant. SPSS (SPSS Inc., Chicago, IL, USA) was used for all calculations and MedCalc┬« version 9.2.0.1 statistical software (MedCalc Software, Mariakerke, Belgium) was used only for comparison between areas under receiver operating characteristic curves of different variables.
RESULTS
General characteristics of the study subjects
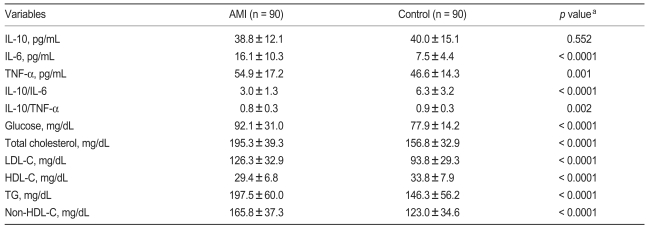
Baseline characteristics of study participants are shown in Table 1. Among these study participants, 90 AMI patients (81 males [90%] and 9 females [10%]) and 90 age-and sex-matched healthy controls (81 males [90%] and 9 females [10%]) were recruited. Individuals who suffered from AMI were more likely to smoke, drink alcohol, suffer hypertension, and have a higher mean waist circumference as compared with healthy controls.
Study population characteristics were compared with controls (Table 2). AMI patients had lower levels of HDL-C and IL-10, and higher fasting glucose, triglyceride, LDL-C, non-HDL-C, total cholesterol, and plasma levels of IL-6 and TNF-╬▒ as compared with control. Furthermore, the ratio of IL-10 to IL-6 and the ratio of IL-10 to TNF-╬▒ were both lower in AMI patients as compared with the control group.
Cytokines
Mean concentrations of anti-inflammatory cytokine IL-10 were lower in the AMI group as compared with the control group; however, this difference was not significant (38.81 vs. 40.03 pg/mL, p = 0.552, Table 2). AMI patients had significantly higher plasma concentrations of the pro-inflammatory cytokines IL-6 and TNF-╬▒ as compared with controls (IL-6 concentration, 16.10 ┬▒ 10.32 vs. 7.52 ┬▒ 4.36 pg/mL; p < 0.0001), (TNF-╬▒ concentration, 54.94 ┬▒ 17.19 vs. 46.61 ┬▒ 14.33 pg/mL; p = 0.001). No significant differences in anti-inflammatory cytokine values were observed; however, the anti- to pro-inflammatory cytokine ratio was significantly lower in AMI patients as compared with controls ([IL-10 to IL-6 ratio, 2.96 ┬▒ 1.31 vs. 6.31 ┬▒ 3; p < 0.0001], [IL-10 to TNF-╬▒ ratio, 0.76 ┬▒ 0.29 vs. 0.91 ┬▒ 0.34; p = 0.002]).
ROC analysis
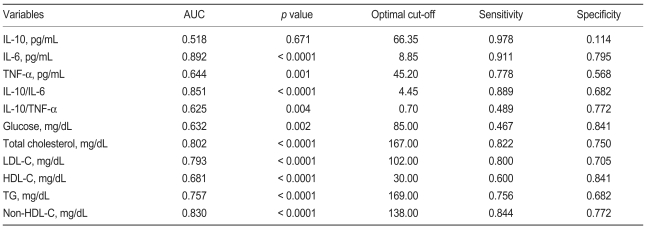
For discrimination between patients and controls, we found that the area under the receiver operating characteristic (ROC) curve ranged from 0.518 to 0.892 (Table 3). As shown in Table 3, IL-6 (area under the curve [AUC], 0.892; p < 0.0001), IL-10 to IL-6 ratios (AUC, 0.851; p < 0.0001), and non-HDL-C (AUC, 0.830; p < 0.0001) showed superior performance against other parameters. IL-6 had the highest area under the curve; however, this value was not significantly higher than the area under the curve for the IL-10 to IL-6 ratio (difference, 0.041; p = 0.069) or non-HDL-C (difference, 0.062; p = 0.111). The area for the IL-10 to IL-6 ratio, which is a balance between anti- and pro-inflammatory cytokine, was slightly larger than the area for non-HDL-C (difference, 0.021; p = 0.615). This analysis demonstrates that IL-6 shows superior performance against the other parameters in our study population. IL-6 concentrations at an optimal cut-off level of 8.85 pg/mL showed a sensitivity and specificity of 91% and 79%, respectively (Table 3). Diagnostic performance and sensitivity and specificity values for other parameters are also shown in Table 3.
Logistic regression analysis
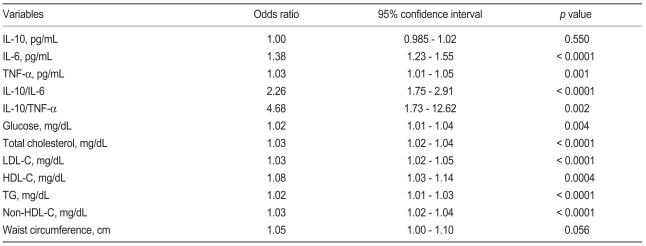
In the univariate logistic regression analysis we found that the ratios of IL-10 to TNF-╬▒ and IL-10 to IL-6 showed greater odds ratios than the other variables (Table 4). To further delineate a potential independent association between IL-6 and TNF-╬▒, a multivariate analysis was performed, which included the ratio of anti- to pro-inflammatory cytokines markers; baseline characteristics, which showed significant discriminating abilities in the ROC curve analysis; and independent variables found in the univariate analysis. Anti- to pro-inflammatory cytokine ratios, TNF-╬▒, LDL-C, and non-HDL-C remained significant. IL-6 was no longer significant (Table 5) after the IL-10 to IL-6 ratio was introduced into the model (odds ratio, 1.38; p < 0.0001 without IL-10 to IL-6 ratio).
DISCUSSION
The assessment of inflammatory markers as additional risk factors in the evaluation of cardiovascular events should be encouraged. Further studies are necessary to determine whether inflammatory markers may represent valid targets for new medications that can be used to slow the atherosclerosis process. Plasma concentrations of cytokines in virtually all of the subjects tested was determined, and it was found that a variety of phenomena were associated with changes in plasma cytokines. In our study, IL-10 to IL-6 cytokines ratios showed more consistent results than any other cytokines.
IL-6 and TNF-╬▒ are known to influence lipid metabolism in animals via two separate mechanisms [13,14]. First, these cytokines stimulate fatty acid synthesis by the liver and secondly, TNF-╬▒ stimulates lipolysis by adipocytes. These changes may explain the association between cytokines and plasma triglyceride. The observation that alcohol consumption is associated with reduced TNF-╬▒ is consistent with studies that have shown suppression of TNF-╬▒ production by macrophages with alcohol consumption [6]. The association of alcohol with reduced plasma TNF-╬▒ may explain the relationship between alcohol and increased HDL-C concentrations.
Circulating IL-6 concentrations may be the result of a variety of stimuli, including various clinical risk factors that lead to the release of IL-6 from numerous cell types, including smooth muscle cells and macrophage/foam cells found in atheromatous plaques [15]. IL-6 can be released from adipocytes and may stimulate a response from the hypothalamic pituitary-adrenal axis, resulting in hypertension and obesity [16]. In this study we also found that increased IL-6 levels are associated with hypertension. Consistent with previous studies [17], we found that circulating levels of IL-6 were increased in obese patients as compared with lean patients. Prior studies of AMI suggest that cytokines are preferentially produced by inflammatory cells in the pre-infarct zone, and persistent elevation of cytokines results from an increased infiltration of inflammatory cells [18]. In our study, individuals with elevated levels of TNF-╬▒ were at an increased risk for AMI. Thus, these data are consistent with the hypothesis that inflammation plays a major role in atherosclerosis [19].
Less information is available regarding the role of anti-inflammatory cytokines in AMI. It recently has been demonstrated that the anti-inflammatory cytokine IL-10 may act as a protective factor in atherosclerosis. IL-10 is expressed in both early and advanced human atherosclerotic plaques [20] and inhibits many cellular processes including metalloproteinase production and tissue factor expression, which may play a role in the clinical expression of atherosclerotic plaque rupture or erosion. IL-10 concentrations were particularly low in the AMI study group. IL-10 is a powerful suppressor of the immune response, and is produced by T-cells, B cells, monocytes, and macrophages [11,21]. IL-10 inhibits pro-inflammatory cytokines such as TNF-╬▒ and IL-6 [11] and has multifaceted anti-inflammatory properties, including inhibition of prototypic pro-inflammatory transcription factors, i.e., nuclear factor ╬║B, which leads to the suppression of cytokine production [22]. IL-10 is expressed in advanced human atherosclerosis and is associated with low inducible nitric oxide synthase expression and low levels of apoptosis [23]. Our study found that plasma IL-10 con-centrations are lower in AMI patients; however, this difference is not statistically significant as compared with the control group. This result suggests that decreased plasma IL-10 concentrations are associated with clinical instability. Pro-inflammatory cytokine (IL-6 and TNF-╬▒) plasma concentrations were significantly higher in AMI patients as compared with controls. In contrast, lower plasma concentrations of the anti-inflammatory cytokine IL-10 were found in the AMI group as compared with controls; however, this difference was not statistically significant. The beneficial effects of elevated IL-10 plasma levels were restricted to patients with elevated IL-6 and TNF-╬▒ plasma levels, which is an indication of an enhanced systemic inflammatory response. These data support the hypothesis that the balance between anti-inflammatory and pro-inflammatory cytokines may reflect the intensity of occult plaque inflammation and vulnerability to rupture [24,25]. Therefore, we examined anti- and pro-inflammatory cytokine ratios and found that IL-10 to IL-6 ratios were strongly associated with AMI. A low IL-10 to TNF-╬▒ ratio is associated with severe malarial anemia, and an insufficient IL-10 response to high TNF-╬▒ concentrations may have had a central role in the progression of this disease [26].
Limitations of previous studies on cytokine markers in AMI include the inclusion of only one or two cytokines that are pro-inflammatory or anti-inflammatory. Multiple cytokines are involved in the inflammatory process, and have overlapping, antagonistic, and synergetic effects on many cell types. In addition, they up-and down-regulate the production of other cytokines and inflammatory markers. In our study, we included two pro-inflammatory cytokines and one anti-inflammatory cytokine. The limitation of the present study is the lack of follow-up data, mostly due to the lack of patient compliance. This additional data may have provided important information about anti- to pro-inflammatory cytokine ratios as markers for risk stratification and prognosis.
In conclusion, inflammation and thrombosis are interconnected pathologies in the natural history of atherosclerosis and measurements of inflammatory markers may aid in predicting the prognosis of patients with AMI. IL-10 to IL-6 ratios and IL-6 measurements were equivalent in their ability to discriminate between persons with and without AMI. Data from the multivariate model, however, suggest that the IL-10 to IL-6 ratio is associated with AMI, whereas IL-6 levels are not. Thus, our data suggest that the IL-10 to IL-6 ratio, and not IL-6 levels, may be a valuable indicator of AMI. Our results also suggest that reduced anti- to pro-inflammatory cytokine ratios may favor atheromatous plaque instability and may be implicated in the development of AMI.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





