


INTRODUCTION
Intractable ascites, severe hyponatremia, and decreased arterial pressure are clinical findings seen in patients with advanced cirrhosis. These conditions occur as a result of high serum levels of renin/aldosterone owing to portal hypertension, a decreased vascular response to vasoactive drugs, and a reduced solute-free water clearance [1-4]. According to several recent studies, hyponatremia occurring as a result of a reduced solute-free water clearance was a key prognostic factor in patients with liver cirrhosis when hyponatremia was incorporated into the MELD score [5-9]. Hyponatremia is a common abnormal finding in approximately 57% of hospitalized patients with chronic liver disease and in 40% of outpatients with liver disease [1,10]. To date, no studies have been conducted to evaluate the prevalence of hyponatremia in Korean hospitalized patients with liver cirrhosis. In fact, no studies have evaluated the association between serum sodium levels and the occurrence and severity of complications due to liver cirrhosis. Given the need for further studies regarding this relationship, we conducted this study to evaluate the prevalence of hyponatremia, to examine whether serum sodium levels correlate with the presence and severity of cirrhotic complications, and to estimate survival rates in patients hospitalized with complications due to liver cirrhosis.
METHODS
Subjects
Patients who were hospitalized with complications due to liver cirrhosis during a 1-year period between 1 January and 31 December 2004 at Ilsan Paik Hospital of Inje University, Korea were included in this study, if a retrospective chart analysis and follow-up telephone call were obtainable. For patient was admitted more than twice during the study period, the medical record of the first admission was collected. A diagnosis of liver cirrhosis was limited to cases with laboratory and clinical findings that met the proper diagnostic criteria [11]. Patients with hepatocellular carcinoma present at admission and during the follow-up period were excluded. Patients using diuretics within a 1-month period before admission and antiviral drugs at any time of survival period were also excluded from the current study. As causative factors for liver cirrhosis, chronic hepatitis B was diagnosed in cases with detectable hepatitis B surface antigen, and chronic hepatitis C was diagnosed in patients positive for anti-HCV antibody. Patients who had ingested alcohol daily at a dose of >80 g for more than 10 years in the absence of other causative factors such as drugs or evidence of a viral infection were defined as having alcoholic liver cirrhosis. Other cases were classified as 'others'.
Study design
Based on the serum sodium concentration measured at the time of admission, patients were divided into three groups: serum sodium Ōēż130 mmol/L, serum sodium between 131 and 135 mmol/L, and serum sodium Ōēź136 mmol/L. Complications included simple ascites, hepatic encephalopathy, spontaneous bacterial peritonitis, hepatic hydrothorax, infection, hepatorenal syndrome, esophageal and gastric varices, upper gastrointestinal bleeding due to varices, and intractable ascites. Ascites, hepatic encephalopathies, and esophageal varices were classified based on severity. Ascites was classified as follows: grade I, ascites observed on imaging study but presence is unclear on physical examination; grade II, ascites easily recognized on gross examination and palpation; and grade III, severe abdominal distention concurrently present on gross examination and large-volume paracentesis performed for therapeutic purposes [12]. Cases of hepatic encephalopathy higher than grade III based on the West Haven criteria were determined to be severe, and other cases were all determined to be mild [13]. Presence of varix was described only the case endoscopic exam was done between 3 month before and after hospitalization. Esophageal varices were classified by size and shape based on endo-scopic findings, as follows: F1, a linear, small sized varix, F2, a beaded, medium sized varix, and F3, a nodular, large varix [14]. Infection was defined in patients hospitalized with infectious diseases except for spontaneous bacterial peritonitis. In cases of hepatic hydrothorax and gastric varices, only the presence of such complications was verified. The concurrent presence of other complications was also examined in accordance with the treatment guidelines of the Korean Association for the Study of the Liver [15]. When death was confirmed on a retrospective analysis of medical records and a telephone interview, the period ranging from the date of hospitalization to death was considered as the survival period.
Statistical analysis
Statistical analysis was performed using SAS. Statistical methods included the Chi-square test and ANOVA. A p value <0.05 was considered statistically significant. To obtain the distribution curve for the survival time depending on the serum sodium concentration at the time of admission, an estimated value of Kaplan-Meier was calculated, and differences in survival time were analyzed using the log-rank test. A hazard ratio for the concurrent presence of complications depending on the severity of hyponatremia was obtained using logistic regression analysis.
RESULTS
Patient characteristics
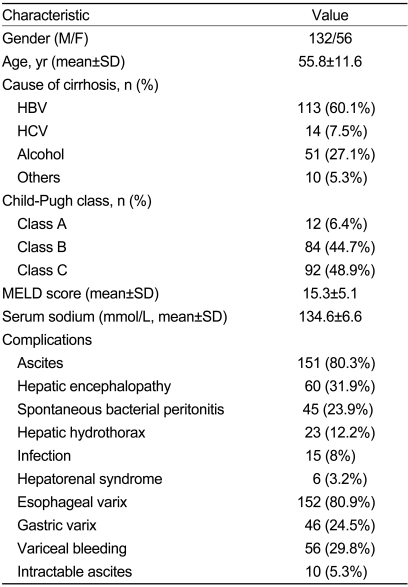
In the current study, we analyzed 188 inpatients with liver cirrhosis who were hospitalized with complications such as simple ascites, spontaneous bacterial peritonitis, intractable ascites, hepatorenal syndrome, hepatic encephalopathy, variceal bleeding, hepatic hydrothorax, and infection. Patients in our series had a mean age of 55.8┬▒11.6 years (range, 29-82 years) and consisted of 132 men (70.2%) and 56 women (29.8%). Causative factors for liver cirrhosis included chronic hepatitis B (113 cases, 60.1%), chronic hepatitis C (14 cases, 7.5%), alcoholic liver disease (51 cases, 27.1%), and other diseases (10 cases, 5.3%). The mean Child-Pugh score was 9.4┬▒1.8 (range, 5-15); the mean MELD score, 15.3┬▒5.1 (range, 5-36); and mean serum sodium concentration, 134.6┬▒6.6 mmol/L (range, 115-147 mmol/L) (Table 1). Based on the diagnostic criteria for hyponatremia in patients with serum sodium concentrations Ōēż135 mmol/L and who were hospitalized with complications due to liver cirrhosis, 90 patients (47.9%) were noted to have concurrent hyponatremia. The proportion of patients with severe hyponatremia (serum sodium, Ōēż130 mmol/L) was 27.1%.
Liver function and concurrent complications based on serum sodium concentration
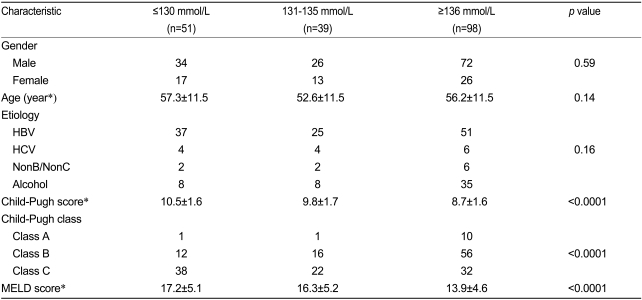
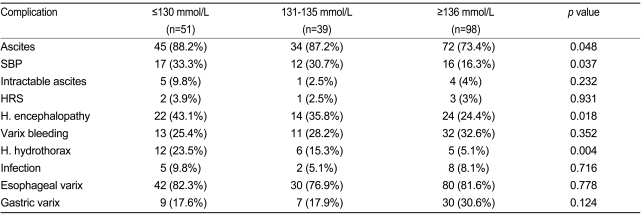
Based on the serum sodium concentration at the time of admission, patients were assigned to three groups: serum sodium Ōēż130 mmol/L (n=51, 27.1%), serum sodium between 131 and 135 mmol/L (n=39, 20.8%), and serum sodium Ōēź136 mmol/L (n=98, 52.1%). There were no significant differences in gender, age, or causative factors for liver cirrhosis among the three groups. The mean Child-Pugh scores for the groups were 10.5┬▒1.6, 9.8┬▒1.7, and 8.7┬▒1.6, respectively, and the mean MELD scores were 17.2┬▒5.1, 16.3┬▒5.2, and 13.9┬▒4.6, respectively. These scores indicate that as hyponatremia became more severe, liver function declined (Table 2). Complications due to liver cirrhosis, including ascites, spontaneous bacterial peritonitis, hepatic hydrothorax, and hepatic encephalopathy, had significantly different frequencies among the three groups, whereas the frequencies of other complications such as intractable ascites, hepatorenal syndrome, variceal bleeding, hepatic hydrothorax, infection, esophageal varices, and gastric varices did not differ significantly among the three groups (Table 3). The severity of ascites and hepatic encephalopathy depending on the serum sodium concentration differed significantly among the three groups, but the severity of varices depending on the serum sodium concentration was not significantly different among the three groups (Table 4).
Risk for developing complications based on serum sodium concentration
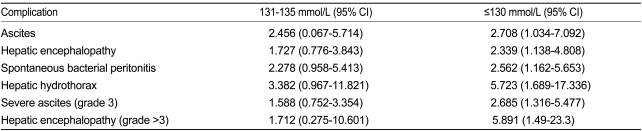
Based on the above results, the risks for developing ascites, spontaneous bacterial peritonitis, hepatic hydrothroax, and hepatic encephalopathy depending on the serum sodium concentration were examined. Patients with a serum sodium concentration Ōēż130 mmol/L, as compared with serum sodium Ōēź136 mmol/L had a significantly increased risk for developing complications: 2.708 (95% CI=1.034-7.092, p=0.043) for ascites, 2.339 (95% CI=1.138-4.808, p=0.021) for hepatic encephalopathy, 2.562 (95% CI=1.162-5.653, p=0.020) for spontaneous bacterial peritonitis, and 5.723 (95% CI=1.689-17.336, p=0.002) for hepatic hydrothorax. Cases with mild hyponatremia (serum sodium between 131 and 135 mmol/L) as compared with serum sodium Ōēź136 mmol/L, had a tendency of increased risk for developing the above complications, although this relationship was not statistically significant (Table 5). Patients with serum sodium concentration Ōēż130 mmol/L, risks of developing severe ascites and hepatic encephalopathy of higher than Grade III were 2.658 (95% CI=1.316-5.447, p=0.007) and 5.891 (95% CI=1.49-23.3, p=0.011). Patients with mild hyponatremia didn't show a statistical significance in the risk for developing severe ascites and hepatic encephalopathy of higher than Grade III. These results indicate an association between the severity of hyponatremia and the risk for developing severe ascites and hepatic encephalopathy (Table 5).
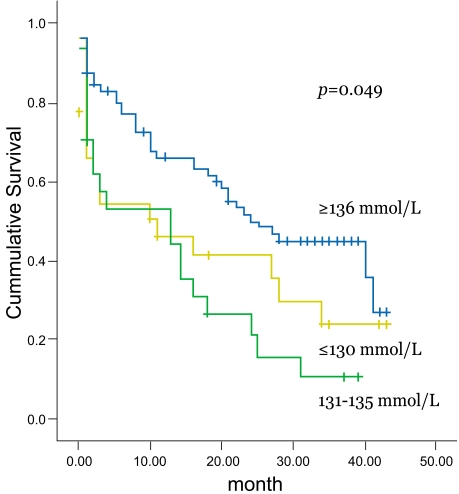
Survival rate according to serum sodium concentration
The 3-year survival rate was 47.2% in patients with a serum sodium Ōēź136 mmol/L, 16.6% in patients with a serum sodium of 131-135 mmol/L, and 33.3% in patients with a serum sodium Ōēż130 mmol/L. The mean survival periods were 24.9, 12.9 and 17.5 months, respectively. The survival rate was significantly correlated with the serum sodium concentration (p=0.0049), (Fig. 1).
DISCUSSION
Hyponatremia is an electrolyte imbalance that commonly occurs in hospitalized patients. Most cases are dilutional hyponatremia caused by the impairment of solute-free water clearance [16]. Hyponatremia resulting from the impairment of solute-free water excretion is commonly accompanied by portal hypertension [10]. In recent years, hyponatremia has attracted interest as a possible prognostic factor for liver cirrhosis. To date, no Korean studies have been conducted to examine its prevalence or the concurrent presence of its complications. We conducted this study to examine the prevalence of hyponatremia and its complications in Korean patients hospitalized with liver cirrhosis.
In a review of a previously conducted multi-center study in overseas countries, 997 patients with liver cirrhosis and concurrent ascites, who were under the care of hepatologists in hepatology outpatient clinics, were assigned to three groups based on serum sodium concentration, in a manner similar to that of the current study. The prevalence of hyponatremia at a serum sodium Ōēż135 mmol/L was 49.4%. Concurrent complications such as severe ascites, impaired renal function, hepatic encephalopathy, spontaneous bacterial peritonitis and hepatorenal syndome, except for gastrointestinal bleeding, occurred with a higher probability in cases of severe hyponatremia (serum sodium Ōēż130 mmol/L) [1]. In a study with 156 patients hospitalized with liver cirrhosis, the prevalence of hyponatremia, based on a serum sodium concentration Ōēż130 mmol/L, was 29.8%, and hyponatremia was significantly correlated with infection and ascites [17]. In the present study, conducted in patients hospitalized with complications due to liver cirrhosis, the prevalence of hyponatremia at a serum sodium concentration Ōēż135 mmol/L was 47.9%, and that of severe hyponatremia at a serum sodium concentration Ōēż130 mmol/L was 27.1%. These results were similar to the overseas reports. In fact, the severity of hyponatremia, particularly at serum sodium concentrations Ōēż130 mmol/L, corresponded to higher risks for developing ascites, hepatic encephalopathy, spontaneous bacterial peritonitis, hepatic hydrothorax, severe ascites, and severe hepatic encephalopathy, compared with the risks in patients with a serum sodium Ōēź136 mmol/L. In agreement with previous reports, serum sodium concentration was not associated with the presence of varices. Furthermore, there was no significant difference in the incidences of hepatorenal syndrome and bacterial infections, except for spontaneous bacterial peritonitis, among the three serum sodium concentration groups. It is possible that no significance was found owing to a lack of statistical power based on the small number of patients with hepatorenal syndrome (n=6) or infection (n=15).
Currently, many ongoing studies are examining the pathophysiology of hyponatremia accompanied by liver cirrhosis, and dilutional hyponatremia has been considered the most plausible pathophysiology [10]. In animal experiments where portal hypertension was induced, the concentration of nitric oxide (NO), with its powerful vasodilatory action, was increased; NO is also increased in patients with portal hypertension. Owing to the vasodilatory effect of increased NO and the lower effective circulating blood volume in these patients, anti-diuretic hormone secretion is facilitated with the mediation of baroreceptors, despite the presence of a hypo-osmotic environment. The increased level of anti-diuretic hormones lowers solute-free water excretion, leading to dilutional hyponatremia [10].
In the current study, the risks for complications such as severe ascites, spontaneous bacterial peritonitis, hepatic hydrothorax, and hepatic encephalopathy were increased at low serum sodium concentrations. With the exception of hepatic encephalopathy, these complications are believed to occur because of increased body fluid resulting from the impairment of solute-free water excretion. Hepatic encephalopathy occurs as a result of severe hepatic dysfunction. In cases in which hyponatremia is concurrently present, however, the increased intracellular concentration of glutamine due to hyperammonemia, along with the adaptation to the hypoosmotic extracellular environment of hyponatremia, increases the severity of hepatic encephalopathy, because organic osmolytes such as myo-inositol become further depleted in the cells [18]. The pathophysiology of hepatorenal syndrome can also be explained by increased body fluid resulting from the impairment of solute-free water excretion. As mentioned earlier, however, our results did not reach statistical significance, probably because only a few patients with hepatorenal syndrome were enrolled in the present study, in contrast to other studies [1,17]. The presence and severity of varices did not correlate with serum sodium concentration in the present study, because development of varices depends on not the excess of body water but the histological changes such as the compression of venules by regenerating nodules, perisinusoidal obstruction resulting from periportal inflammation, or fibrosis and decreased sinusoidal elasticity and diameter caused by collagen deposition in the space of Disse. Further studies are needed to demonstrate a significant relationship between the serum sodium concentration and the above histological changes.
MELD scores were initially designed to predict survival in patients who underwent elective placement of a transjugular intrahepatic portosystemic shunt and are currently used as an indicator of mortality in patients with liver cirrhosis [19]. MELD scores are advantageous for objectively predicting mortality in a homogeneous manner because their constituent variables are objective [20]. However, MELD scores have the disadvantage of not reflecting the early deaths in patients with lower MELD scores [2]. Many studies have been conducted recently to examine the clinical usefulness of MELD-Na scores using the serum sodium concentration as a prognostic indicator. In the clinical setting, MELD-Na scores may be more useful than MELD scores for the allocation of livers for transplantation and for the prediction a short-term death [21,22]. The clinical significance of the serum sodium concentration was demonstrated in a retrospective study that looked for factors associated with death prior to liver transplantation in 507 patients with liver cirrhosis and lower initial MELD scores. The persistent presence of ascites and hyponatremia were independent risk factors in patients with MELD scores lower than 21 points, and MELD scores were a prognostic indicator only in other patients [2]. In the current study, there was a significant difference in the 3-year survival rate among the three serum sodium concentration groups. However, the 3-year survival rate was higher in patients with serum sodium concentration Ōēż130 mmol/L than in those with serum sodium concentration between 131 and 135 mmol/L. These results indicate that the serum sodium concentration alone cannot predict the survival rate in patients with liver cirrhosis and that factors other than the serum sodium concentration affect patient survival. Further large-scale studies are warranted to explore these factors.
One limitation of the current study was that it did not assess the effect of serum sodium concentration on the risks for developing complications but simply examined the concurrent presence of complications and sodium levels in a retrospective analysis. Further prospective studies are needed to determine the clinical significance of hyponatremia and to identify its correlation with the incidence of possible complications.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





