


INTRODUCTION
Eosinophilic or hypersensitivity myocarditis is a relatively rare condition; it is usually caused by drugs (most commonly penicillin, sulfonamides, diuretics, and methyldopa) or parasites1). It sometimes occurs in patients with comorbid allergic disorders or hypereosinophilic syndrome, and is associated with peripheral eosinophilia2, 3). However, in some cases there are no identifiable allergens. This type of myocarditis clinically resembles viral myocarditis, and is therefore rarely recognized without endomyocardial biopsy.
We present a case of acute eosinophilic myopericarditis, who presented with cardiogenic shock, and was diagnosed by endomyocardial biopsy in the early stage4, 5), with normal peripheral eosinophil count at the time of endomyocardial biopsy in a 25 year-old woman without known allergy or history of drugs. The patient recovered without sequelae.
CASE REPORT
A 25 year-old woman was transferred to the The Heart Center of Chonnam National University Hospital because of shortness of breath and hypotension for one day. Four days before admission, the patient complained of fever and sore throat, but took no medications. Three days earlier, the patient had nausea, vomiting, loose stools, lower abdominal pain and a general feeling of weakness. The patient visited a local clinic and was admitted for conservative treatment for acute gastroenteritis. At that time of admission, her body temperature was normal and blood pressure was 100/60 mmHg. On hospital day 2, the patient complained of feeling dizzy, had chest discomfort and progressive shortness of breath; the blood pressure dropped to 80 mmHg in systole. The patient was then transferred to our hospital.
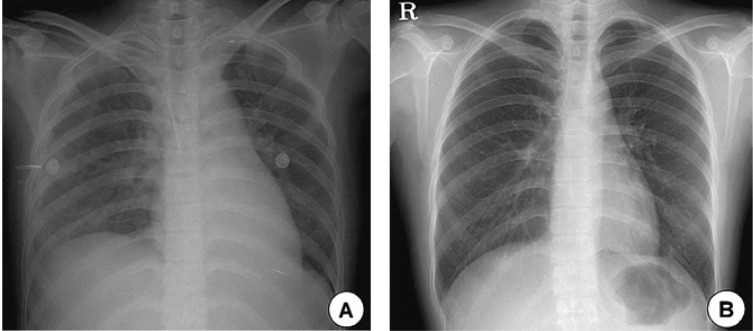
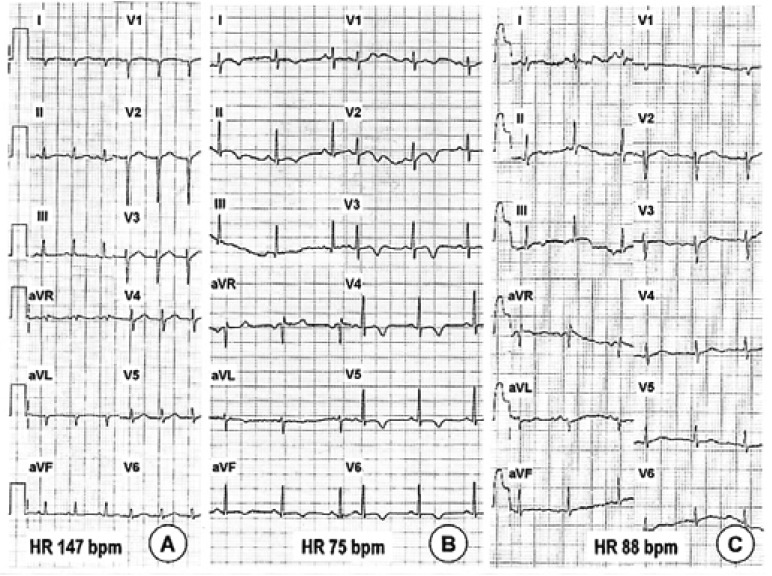
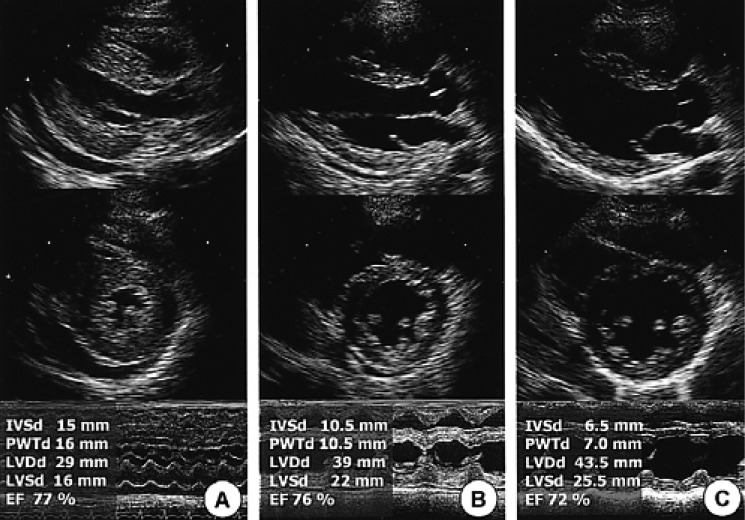
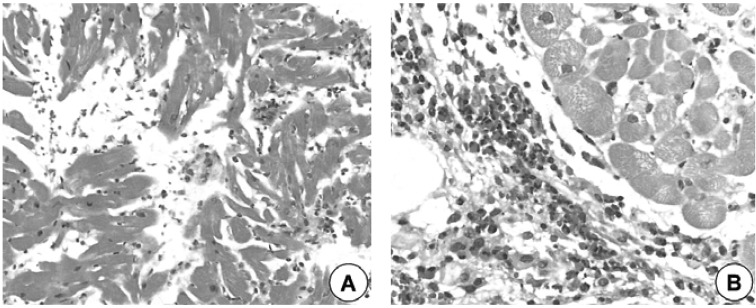
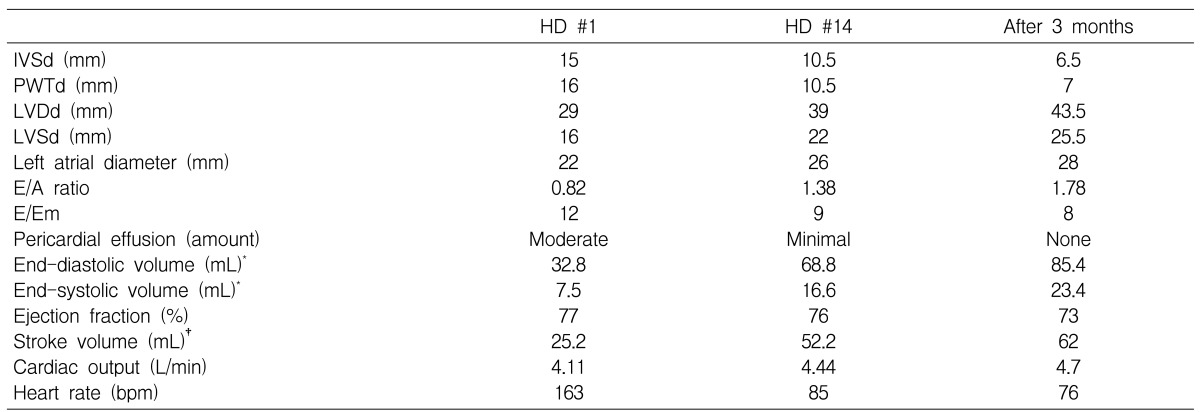
The patient was a student and resided in a local area. There was a history of occasional alcohol. There was no history of smoking, drugs or allergies prior to admission. On physical examination, the patient was drowsy, but oriented, and had shortness of breath. The blood pressure was 85/40 mmHg with a continuous intravenous infusion of dopamine (15 ┬Ąg/kg/min) and norepinephrine (0.02 ┬Ąg/kg/min), the pulse 150 beats per minute, the respiratory rate 24 breaths per minute, and the body temperature 36Ōäā. The oxygen saturation was 100 percent with oxygen supplied at 3 L/min by nasal cannula. The lung sounds were coarse on both lower lung fields, the heart was rapidly beating without murmur, and the r neck veins were slightly engorged. The skin was cool and clammy, but had no eruption, and no pitting edema. The remainder of the physical examination including neurological examinations revealed no abnormalities. The laboratory findings showed a complete blood count with increased white blood cells (17,500/mm3 (neutrophil 75%, eosinophil 2.6%)) and normal hemoglobin (12.7 g/dL), hematocrit (37.9%), and platelet count (267,000/mm3). Blood chemistries showed the following: aspartate aminotransferase 299 U/L, alanine aminotransferase 422 U/L, alkaline phosphatase 44 U/L, total protein 5.6 g/dL, albumin 3.0 g/dL, and lactate dehydrogenase 1,226 U/L, blood urea nitrogen 26.7 mg/dl, creatinine 1.2 mg/dL, amylase 23 U/L, sodium 135 mEq/L, and potassium 4.1 mEq/L. Cardiac enzymes were elevated (myoglobin 148 ng/mL, creatine kinase 215 U/L, CK-MB 14.3 U/L, troponin I 4.49 ng/mL), and NT-proBNP >35,000 pg/mL and C-reactive protein 9.0 mg/dL were also increased. A chest radiograph revealed increased pulmonary vascular markings and a normal cardiac silhouette (Figure 1). Electrocardiogram revealed a sinus tachycardia (heart rate 147 bpm), low voltage and right axis deviation, but no definite ST-T change was noted (Figure 2). Titers of serum neutralizing antibodies for coxsackievirus, adenovirus, Epstein-Barr virus, cytomegalovirus, herpes virus, hepatitis B and C virus, and HIV were all negative. Echocardiography demonstrated a mild hypokinesis of left ventricular (LV) anteroseptal wall with LV wall thickening, and hyperdynamic LV function with reduced stroke volume, moderate amount of pericardial effusion, dilated inferior vena cava with increased hepatic echogenicity, and no significant valvular abnormalities (Figure 3, Table 1). The endomyocardial biopsy specimen from the right ventricle revealed extensive interstitial edema associated with focal necrosis of myocytes, diffuse infiltration of inflammatory cells with lymphocytes, neutrophils, and eosinophils suggesting acute eosinophilic myocarditis (Figure 4). Skin tests for allergy and stool ova were negative.
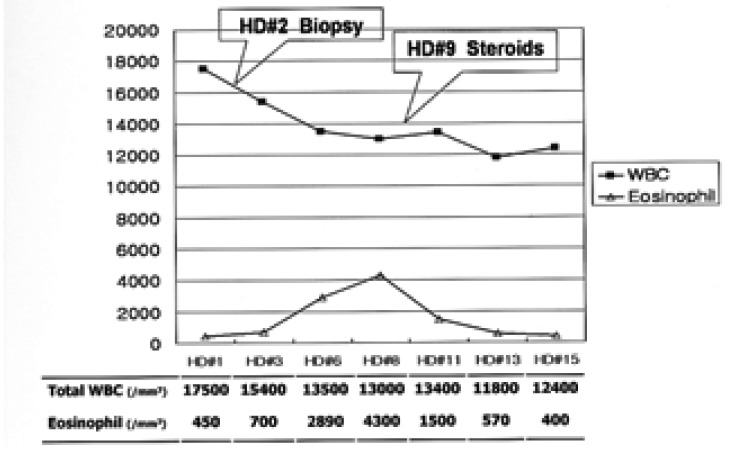
With conservative treatment, the blood pressure was normalized on day 3 after the admission, and the cardiac enzymes were also normalized during the hospitalization. However interestingly, the peripheral blood eosinophil count increased through hospital day 8, from an initial count 450/mm3 to peak 4,300/mm3 (Figure 5). The patient complained of chest pain on motion, and the electrocardiogram was sinus rhythm with T inversions on all leads (Figure 2), but no definite friction rub was auscultated. We treated the patient with oral prednisolone, 1 mg/kg of body weight, for the symptoms of pericarditis and it subsided 2 days later. Blood eosinophil count was normalized over 6 days after administration of steroids. The follow up chest radiograph was clear, (Figure 1) and the echocardiography showed good LV wall motion and function with decreased LV wall thickening and normal LV cavity size, and a minimal amount of pericardial effusion remaining (Figure 3, Table 1). The patient was discharged and followed up at the outpatient clinic with a tapering dose of prednisolone over next 3 months. After 3 months, the electrocardiogram had returned to normal, and the pericardial effusion cleared (Figure 2, 3).
DISCUSSION
In this case of eosinophilic myopericarditis, there are several clinical features that are similar with common viral myocardits, e.g., hemodynamic collapse of sudden onset, preceding history of upper respiratory infection, elevated cardiac enzymes and increased systemic inflammatory markers.
In many cases, peripheral eosinophilia is observed, but the peripheral blood eosinophil count was normal in this case at the time of presentation, and there was no identifiable cause of the hypersensitivity and no known past history of allergy or drugs in this case. At the local clinic, the initial treatment did not include any drugs known for causing myocarditis, such as antibiotics, anticonvulsants, or diuretics. Medication administered intravenously included metoclopramide and scopolamine. This phenomenon, i.e., acute eosinophilic myocarditis with normal peripheral eosinophil count, has been reported6-8). Morimoto et al.6) reported that in the early stage of eosinophilic myocarditis, peripheral hypereosinophilia is not present initially in some patients, and may not develop during the course of the illness in a subset of these patients.
Treatment of eosinophilic myocarditis is usually conservative. The effectiveness of corticosteroids treatment has not been proven; however, some studies advocate that early administration of high-dose corticosteroids is necessary because acute fulminant eosinophilic myocarditis is usually fatal and diagnosed at autopsy. Some patient improves instantly and dramatically after corticosteroid therapy5, 7, 9). However, we are not sure whether clinical and echocardiographic improvements in this case were an effective response to corticosteroids or the natural course of the disease, because the prednisolone was administered rather late in the course of recovery from pericarditis symptoms.
In conclusion, we present a case of acute eosinophilic myopericarditis presenting with cardiogenic shock, diagnosed by endomyocardial biopsy at an early stage when the peripheral eosinophil count was normal, but increased later. The patient recovered completely and no identifiable cause of hypersensitivity was determined.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





