


INTRODUCTION
Primary squamous cell carcinoma of the thyroid is an extremely rare tumor that accounts for less than 1% of all primary thyroid carcinomas1-3). The disease is usually detected in patients in the age range of 50 to 70 years at the time of presentation4, 5). and shows no sex predilection1, 6). A normal thyroid has no squamous cells; however, a diseased thyroid may contain them. Primary squamous cell carcinoma of the thyroid may develop from squamous metaplasia of the follicular epithelium in a variety of pathologic conditions, such as, other differentiated carcinomas of the thyroid1, 6, 9-14). Thyroid carcinoma commonly presents as sudden enlargement of a neck mass with associated pressure symptoms. At presentation, tumors have usually invaded adjacent tissues and lymph nodes or have metastasized more widely. Primary squamous cell carcinoma of the thyroid is considered a lethal tumor, with an aggressive course similar to that of anaplastic thyroid carcinoma. The median survival of patients with this diagnosis is usually less than one year. To date, there are only three cases reported of patients remaining alive more than six years after diagnosis5). We report here on a patient with primary squamous cell carcinoma of the thyroid who remains alive more than 8 years after diagnosis.
CASE REPORT
A 56-year-old man presented with a hoarse voice and a rapidly progressive mass on the right side of his thyroid gland that had developed over the previous three months. He had no clinical symptoms related to thyroid dysfunction. There was no history of radiation exposure to the neck and no family history of thyroid cancer. Five years earlier, he had been diagnosed with a carcinoid tumor in the left lobe of the lung by percutaneous biopsy at another hospital; the patient has been asymptomatic throughout the prior five-year period.
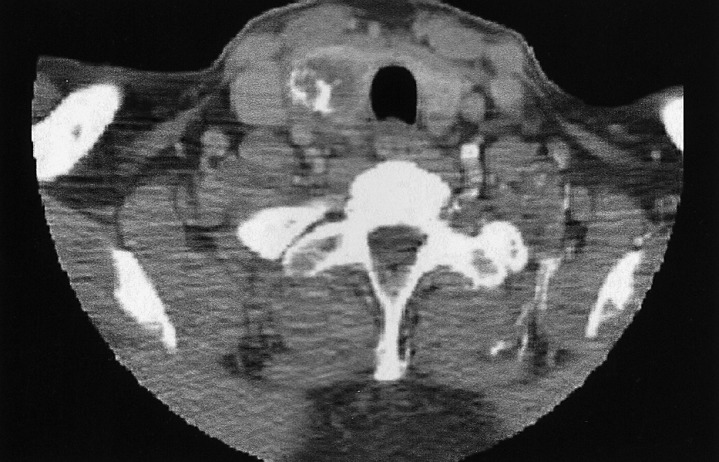
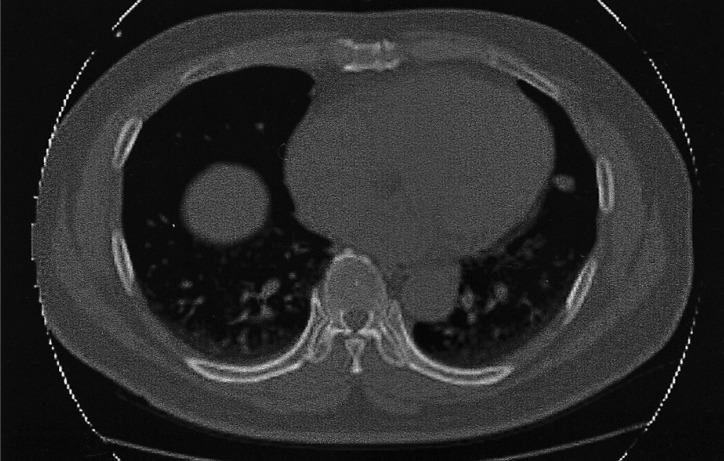
A physical examination revealed a hard, non-tender mass with a maximum transverse diameter of 3 cm on the right side of the thyroid gland. Palpable lymphadenopathy was absent in the cervical and supraclavicular area, and a laryngoscopic examination showed no abnormal findings from the oral cavity to the larynx. Laboratory examination showed a serum TSH level of 3.22 mU/L (reference range 0.30~5.00), T3 1.66 nmol/L (0.92~2.78), T4 78 nmol/L (58~140), anti-thyroglobulin antibody 1 U/mL (0~100), anti-microsomal antibody 1 U/mL (0~100), and thyroglobulin 170.1 ng/mL (0~25). There were no abnormal findings on the hematologic and biochemical laboratory tests. Neck computed tomography (CT) showed a low attenuated, calcified mass with a maximum diameter of 3 cm on the right side of the thyroid gland (Figure 1). An ultrasonography-guided fine needle aspiration and cytology (FNAC) showed a small number of benign follicular cells without atypical cells. Chest X-ray and CT showed a 1 cm sized nodule in the upper lingular segment of the left lung; this nodule was previously diagnosed as a carcinoid, and was noted to have decreased in size. However, three small nodules were newly detected in the left lower lobe of the lung by comparison with prior films (Figure 2). The new nodules noted in the left lower lobe of the lung were diagnosed as follicular neoplasm by FNAC.
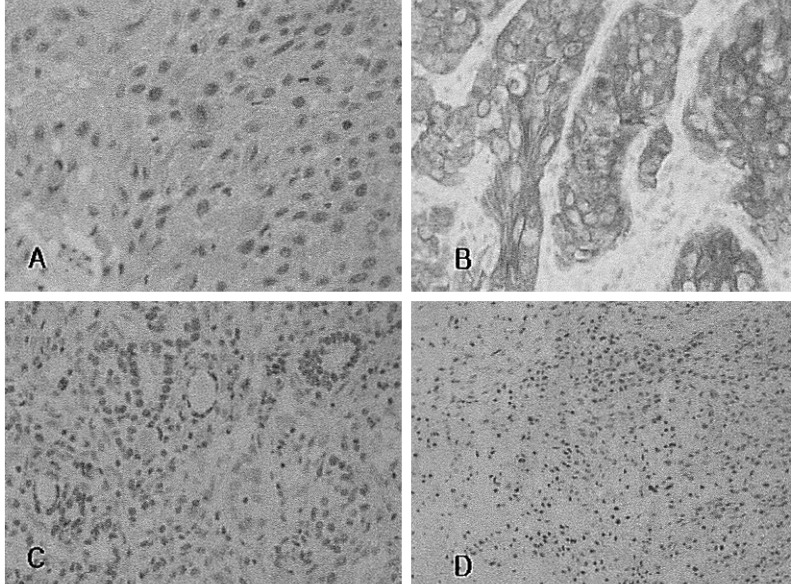
The patient underwent a total thyroidectomy without neck lymph node dissection for the presumed diagnosis of follicular thyroid carcinoma with lung metastasis. However, the histopathologic evaluation revealed a well-differentiated squamous cell carcinoma 3 cm by 3 cm in size in conjunction with follicular carcinoma (Figure 3A). Intermingled and transitional zones of squamous cell carcinoma and follicular carcinoma were present. The tumor was confined to the thyroid gland with internal necrosis and dystrophic calcification. Immunohistochemical staining for cytokeratin 19 was strongly positive for squamous cell carcinoma and negative for follicular carcinoma (Figure 3B). Immunohistochemical staining for thyroglobulin and thyroid transcription factor-1 (TTF-1); was positive for follicular carcinoma and negative for squamous cell carcinoma (Figure 3C, 3D).
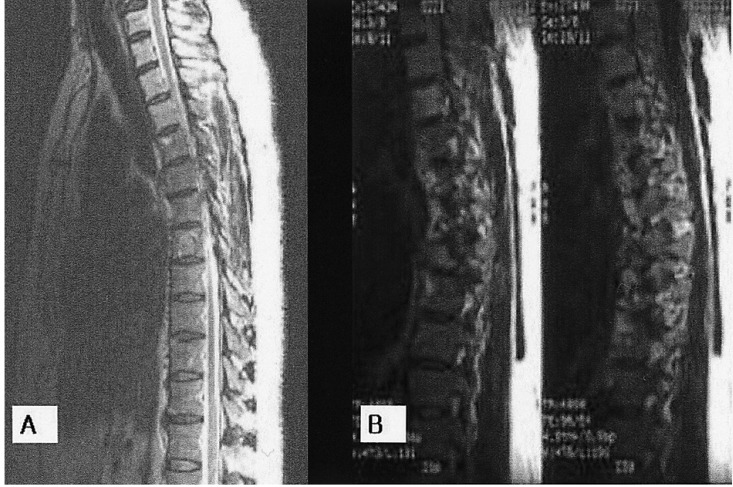
Two weeks after surgery, a 18F-FDG whole body positron emission tomography (PET) was performed and abnormal uptake was identified in a right submandibular lymph node, bilateral jugulodigastric lymph nodes, T7 spine, and lingular segment of the left upper lung; these findings favored the presence of a malignancy. Magnetic resonance imaging (MRI) also demonstrated a Bull's eye lesion with slight enhancement at the T7 vertebral body, suggesting metastasis (Figure 4A). Metastatic squamous cell carcinoma was excluded by laryngoscopy, esophagogastroscopy, abdominal ultrasonography, neck and chest CT, and whole body PET. The patient underwent 5000 rads of adjuvant radiotherapy to the neck postoperatively. Considering the poor prognosis for patients with primary squamous cell carcinoma of the thyroid, we did not pursue a further work-up or aggressive treatment. The patient was treated with TSH suppressive therapy with 200 ┬Ąg of L-thyroxine only.
Three years later, lower extremity paraplegia suddenly developed after the patient had a fall. The thoracic spine MRI demonstrated a metastatic lesion with a compression fracture and an epidural mass formation at the T7 spine, and other newly appeared metastatic lesions on T1, T4, T5, T6 and T8 (Figure 4B). These lesions were treated with external radiotherapy. The patient seemed to have almost completely recovered from paraplegia after radiotherapy. At that time, a chest X-ray showed that the pre-existing nodules noted in the left lower lobe of the lung had increased in size, and that multiple nodules were newly present in the right upper lobe of the lung. Serum thyroglobulin levels were increased to 423.2 ng/mL on T4 suppression therapy.
Seven years later, colon cancer was detected. A preoperative chest CT showed multiple new nodules in the left lower lobe of the lung. Percutaneous biopsy directed to a new nodule in the left lower lobe of the lung was undertaken, and histopathologic findings revealed metastatic follicular carcinoma originating from the thyroid. High dose radioactive iodine therapy was administered after the patient underwent colectomy for colon cancer. At that time, the serum thyroglobulin level was 530.7 ng/mL and the anti-thyroglobulin antibody titer was 1 U/mL on the T4 suppression therapy. The patient now remains alive in satisfactory condition more than eight years after being diagnosed with primary squamous cell carcinoma of the thyroid. Recently, his serum thyroglobulin level had increased to 1164 ng/mL on T4 suppression therapy.
DISCUSSION
Primary squamous cell carcinoma of the thyroid has a remarkably aggressive clinical course, and median survival is usually less than one year. To date, approximately 130 cases of primary squamous cell carcinoma of the thyroid have been reported in the English literature1-6, 9-14). In Korea, nine patients with primary squamous cell carcinoma of the thyroid have been reported15-22). Of these reported patients, only three have survived more than six years after diagnosis5). Cook et al. reported 16 patients with primary squamous cell carcinoma of the thyroid who underwent thyroidectomy between 1936 and 1997. Among these, a 69-year-old woman lived for 16 years after the initial diagnosis. In addition, a 78-year-old and a 55-year-old woman died from heart failure 6 and 21 years after diagnosis, respectively. All reported patients had undergone complete tumor excision and had received 60 Gy of external radiotherapy to the neck. The squamous cells of squamous cell carcinoma have no affinity for iodine as they do not possess intracellular TSH receptors11). and thus, radioactive iodine and TSH suppression therapy have little impact on its clinical course6, 9, 10). Most primary squamous cell carcinomas of the thyroid recur postoperatively and complete tumor excision is the only curative modality; although external radiation therapy to the neck likely has a role as postoperative adjuvant therapy5, 9).
In the present case, a thyroid tumor had already metastasized to the adjacent cervical lymph nodes, lung, and spine at diagnosis. However, the clinical course was indolent and thus differed from that of classical squamous cell carcinoma previously reported. Seven years later after diagnosis, a lung biopsy revealed that the lung lesion was a metastatic follicular carcinoma originating from the thyroid. In view of this slow progression, we believe that the primary thyroid squamous cell carcinoma had been completely excised at thyroidectomy, and that the metastatic lesions were follicular carcinomas from the thyroid; however, only the lung lesion was found to be metastatic follicular carcinoma.
Metastatic thyroid carcinoma accounts for only 0.05~3.9% of all malignant thyroid tumors23, 24), and usually originates from the direct invasion of laryngeal, tracheal or esophageal carcinoma, or as a result of distant metastasis from hypernephroma, breast, lung or gastrointestinal tract carcinoma23, 25, 26). In the present case, the possibility of metastatic squamous cell carcinoma was excluded by laryngoscopy, esophagogastroscopy, abdominal ultrasonography, neck and chest CT, and whole body PET.
The thyroid gland does not usually contain squamous epithelium. Thus, it is not clear how a squamous cell carcinoma develops within the thyroid. One theory proposes that squamous cells are derived from various embryonic remnants, such as, the thyroglossal duct structures, thymic epithelium, and ultimobranchial remnants27-29). However, an alternative theory is more commonly accepted. This suggests that squamous metaplasia occurs in the follicular epithelium as a result of chronic inflammation or scarring in the thyroid; this squamous metaplasia facilitates the development of squamous cell carcinoma in affected epithelium1, 6, 9-14). Sahoo et al. reported two cases of primary squamous cell carcinoma of the thyroid that stained positive for thyroglobulin; this suggested that squamous cell carcinoma of the thyroid might originate from the follicular epithelium of the thyroid. However, no other cases of squamous cell carcinoma of the thyroid, staining positive for thyroglobulin, have been reported (including the present case). Occasionally, primary squamous cell carcinoma of the thyroid occurs in association with other thyroid diseases such as adenomatous goiter, Hashimoto's thyroiditis, papillary carcinoma, follicular carcinoma, medullary carcinoma and anaplastic carcinoma3, 9, 30, 31). These findings, and those of our case, support the latter theory, i.e., that squamous metaplasia and carcinoma develop in a thyroid with underlying disease.
In thyroid cancers, immunohistochemical staining for cytokeratin 19 has been found to be strongly and diffusely expressed in papillary carcinoma of the thyroid32) as well as in squamous cell carcinoma; however, it is infrequently expressed in follicular carcinoma14). TTF-1 is a tissue-specific transcription factor expressed in thyroid follicular cells, that is thought to contribute to the maintenance of a differentiated phenotype33). Immunohistochemical staining for TTF-1 and thyroglobulin are usually expressed in normal thyroid tissues and well-differentiated carcinoma. However, TTF-1 and thyroglobulin are not expressed in undifferentiated carcinoma34). The immunohistochemical staining identified in our patient showed typical findings consistent with the diagnosis of squamous cell and follicular cell carcinoma.
Additional pathology important for consideration as part of the differential diagnosis of primary squamous cell carcinoma of the thyroid include: squamous metaplasia and CASTLE (carcinoma showing thymus-like differentiation)14). If squamous metaplasia is severe, or occurs in association with another thyroid malignancy, pathologists may have difficulty differentiating it from squamous cell carcinoma8, 10). CASTLE is a thymic carcinoma found within the thyroid and frequently has squamous differentiation, as first described in 198535). The clinical behavior of this condition is usually mild, and recurrence after surgery is less frequent than that of squamous cell carcinoma36).
Three experienced pathologists in our hospital reviewed and discussed this pathology several times over the eight years of follow up of this patient. The diagnosis was doubted because of the patient's good clinical course despite the usual aggressive nature of squamous cell carcinoma. However, the pathologists continue to agree with the diagnosis of squamous cell carcinoma of the thyroid different from squamous metaplasia or CASTLE.
We report a case of primary squamous cell carcinoma of the thyroid combined with follicular thyroid carcinoma; the patient remains alive and stable more than eight years after diagnosis.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





