


INTRODUCTION
Human gastric cancers may be histologically divided into two main groups, the intestinal type and the diffuse type, as proposed by Lauren's classification system1). As has been proposed by the Japanese Research Society for Gastric Cancer2), these two types roughly correspond to the differentiated and undifferentiated types, respectively, according to the degree of glandular formation exhibited by the tumor cells. Although these classifications have been widely used, they are inadequate for research regarding the histogenesis of gastric carcinomas and phenotype expression at the cellular level. This is largely due to the confusion of intestinal phenotypic cancer cells with "diffuse" structure and the presence of a gastric phenotype with the "intestinal" type of Lauren's classification3). With respect to the histogenesis of these two types of gastric carcinoma, differentiated-type tumors have generally been considered to arise from gastric mucosa with intestinal metaplasia. It has generally been believed that undifferentiated-type tumors arise from originary gastric mucosa without intestinal metaplasia. These two types of tumor are known to follow different genetic pathways during carcinogenesis4, 5).
Analysis of the phenotypic expression of each gastric cancer cell is possible through the use of cell markers from the gastric and intestinal epithelia6-12). Independent of histological type, human gastric cancers at an early stage mainly consist of malignant cells of the gastric phenotype, while their advanced counterparts tend to have more malignant cells of the intestinal phenotype with progression6, 11, 13, 14). It has been reported that differentiated-type gastric carcinomas of the gastric phenotype (G-phenotype) are more likely to transform into undifferentiated-type carcinoma and show infiltrative growth into the deeper layers of the mucosa or invasion of the surrounding structures9, 15, 16). Eodoh et al.15) detected an E-cadherin gene mutation in 21% (4/19) of the differentiated-type carcinomas of the G-phenotype, although this mutation has generally been considered to be involved in undifferentiated-type carcinomas, and not differentiated-type. The aforementioned study speculated that differentiated-type carcinomas of the G-phenotype progressed to undifferentiated-type carcinomas through the loss of the E-cadherin function and that the biological behavior of this type of tumor was particularly aggressive15).
It is now clear that, in terms of the gastric and intestinal phenotypic marker expression pattern of the tumor, gastric carcinomas can be of various types6, 7). With respect to the clinicopathologic significance of the gastric and intestinal phenotypic marker expression pattern of gastric carcinomas, Koseki et al.9) reported the G-phenotype to be an independent factor associated with lymph node metastasis among differentiated-type early gastric carcinomas. However, several authors10, 17-22) have demonstrated a correlation between the prognosis and the phenotypic markers in gastric cancers. Still, concrete conclusions have yet to be drawn.
Therefore, in order to investigate the clinicopathologic significance of gastric and intestinal phenotypic marker expression patterns among the gastric carcinomas, we examined surgically resected tumor specimens from 343 patients with gastric carcinoma by immunohistochemical staining with monoclonal antibodies CLH2 (ant-MUC5AC), CLH5 (anti-MUC6), Ccp58 (anti-MUC2), and 56C6 (anti-CD10).
MATERIALS AND METHODS
Patients
We examined 343 primary gastric cancer specimens that had been surgically resected at Pusan National University Hospital, Pusan, Korea, from January 2002 and June 2004. The participants in this study included 235 men and 108 women, aged 58.0±11.2 years (mean±standard deviation). No preoperative radiotherapy or chemotherapy had been administered to these patients.
Clinicopathologic review
All specimens were fixed in 10% buffered formalin. Carcinomas with adjacent non-neoplastic mucosa were serially cut into 5-mm slices in parallel with the lesser curvature and embedded in paraffin. These were then sectioned and stained with hematoxylin-eosin for histological examination. Carcinomas were classified by Lauren's classification1). Clinicopathologic findings such as age, gender, tumor site, tumor size, histologic type, depth of invasion, lymphatic invasion, blood vessel invasion, perineural invasion, and lymph node metastasis were reviewed according to the Japanese Classification of Gastric Carcinomas2).
Immunohistochemistry
We examined the expression of MUC5AC, MUC6, MUC2, and CD10 in carcinoma cells by immunohistochemistry (Table 1), as previously described3, 9, 10, 23, 24). Briefly, 4 m-thick consecutive sections were deparaffinized and hydrated through a graded series of alcohol. After inhibition of endogenous peroxidase activity by immersion in 3% H2O2/methanol solution, antigen retrieval was carried out with 10 mmol/l citrate buffer (pH 6.0) in a microwave oven for 10 minutes at 120℃. The sections were then incubated with the primary antibodies. Next, subsequent to thorough washing in phosphate-buffered solution (PBS), the sections were incubated first with biotinylated secondary antibody, and then with avidin-biotinylated horseradish peroxidase complex (Vectastain Elite ABC kit, Vector Laboratories30, Burlingame, Calif., USA). Finally, the immune complexes were visualized by incubation with 0.01% H2O2 and 0.05% 3,3-diaminobenzidine tetrachloride (DAB). Nuclear counterstaining was accomplished using Mayers hematoxylin.
The results of each antibody staining were evaluated with reference to the percentage of positively-stained cancer cells. A result was considered positive if at least 10% of the cells were stained. When less than 10% of cancer cells were stained, the results of immunostaining were considered negative.
Classification of mucin phenotype
MUC5AC and MUC6 are markers of gastric epithelial cells, whereas MUC2 and CD10 are typical of the intestinal epithelial cell phenotype3, 9, 10, 25). Gastric cancers in which more than 10% of the section area consisted of at least one gastric or intestinal epithelial cell phenotype were classified as G-phenotype or I-phenotype cancers, respectively. Those which exhibited both gastric and intestinal phenotypes were classified as gastric and intestinal mixed phenotype (GI-phenotype) cancers, while those showing neither gastric nor intestinal phenotype expression were grouped as cancers of the null phenotype (N-phenotype).
Statistical analysis
The data were analyzed for differences between the groups using Student's t-test, Fischers exact test, or χ2 test. Values of p<0.05 were considered statistically significant. Statistical calculations were performed with SPSS version 10.0 for Windows software (SPSS Inc., Chicago, IL, USA).
RESULTS
Gastric and intestinal phenotypic marker expression in 343 gastric carcinomas
The expression of MUC5AC, MUC6, MUC2, and CD10 was demonstrated in 182 (53.1%), 60 (17.5%), 157 (45.8%), and 61 (17.8%) of the 343 gastric carcinomas, respectively (Figure 1). Taking into account the combinations of expression of these four markers, the 343 gastric carcinomas were respectively classified into G-phenotype tumors (114; 33.2%), GI-phenotype tumors (88; 25.7%), I-phenotype tumors (92; 26.8%), and N-phenotype tumors (49; 14.3%).
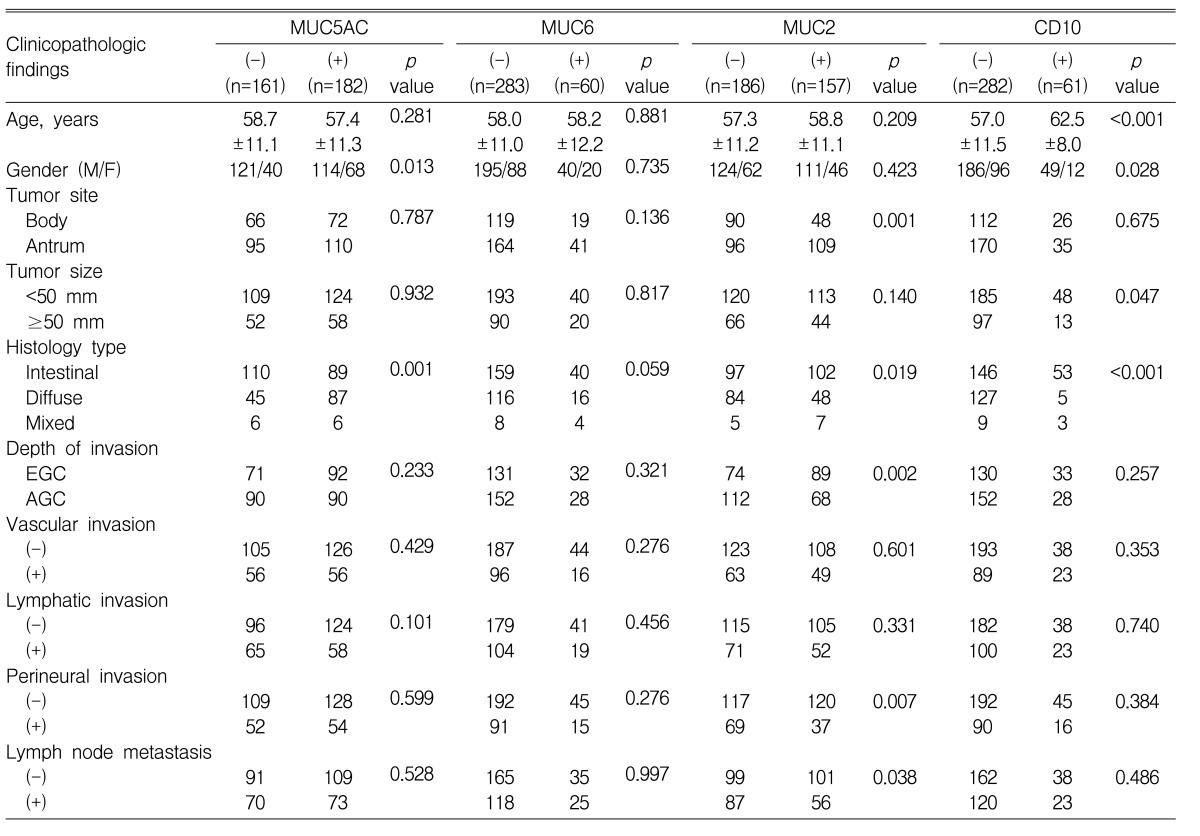
Correlations between clinicopathologic findings and MUC5AC, MUC6, MUC2, and CD10 expression in 343 gastric carcinomas
The correlations between the clinicopathologic findings and the expression of MUC5AC, MUC6, MUC2, and CD10 in the 343 gastric carcinoma patients are shown in Table 2. MUC5AC expression was associated with a lower male-to-female ratio and a higher proportion of diffuse-type tumors (p=0.013 and p=0.001, respectively). No significant correlations were observed between MUC6 expression and any of the variables examined. MUC2 expression was correlated with a higher proportion of antral location, intestinal-type tumors, and early gastric cancers (p=0.001, p=0.019, and p=0.002, respectively). It was also associated with lower proportions of perineural invasion and lymph node metastasis (p=0.007 and p=0.038, respectively). CD10 expression was correlated with a higher mean patient age, a higher male-to-female ratio, and a higher proportion of intestinal-type tumors (p<0.001, p=0.028, and p<0.001, respectively).
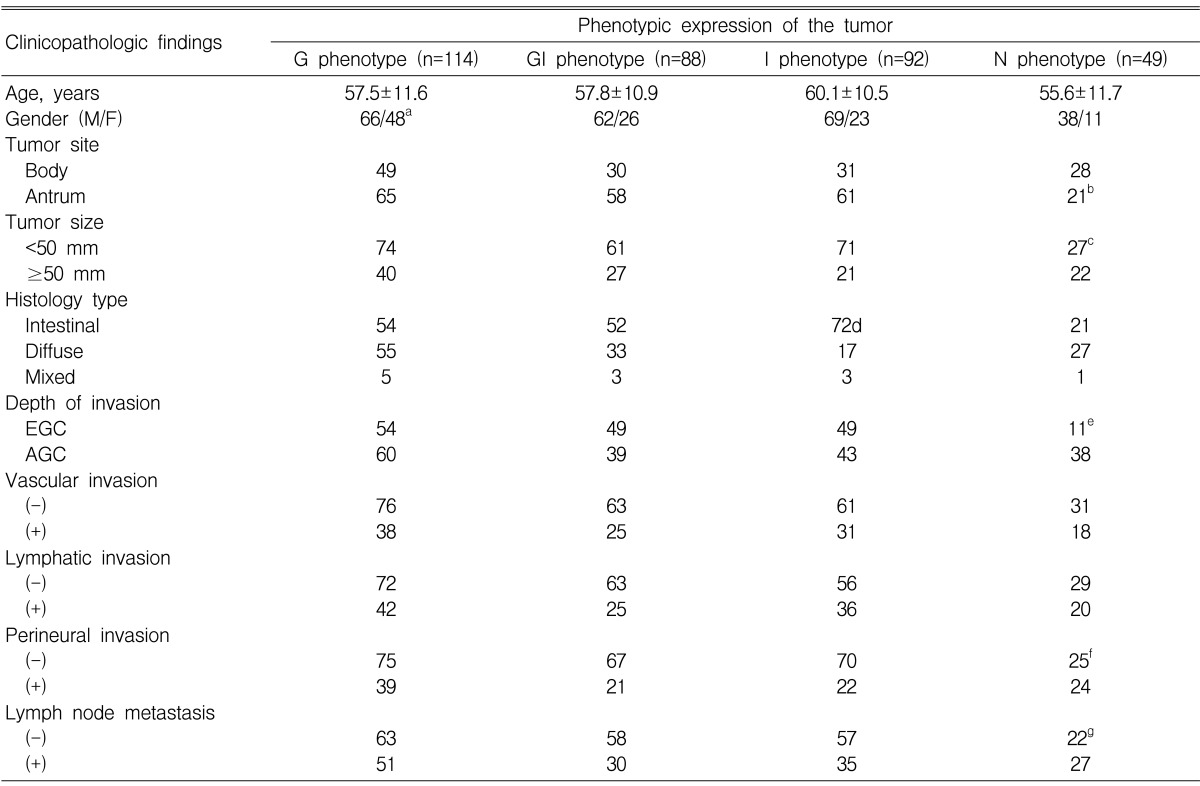
Correlations between clinicopathologic findings and phenotypic marker expression patterns in 343 gastric carcinomas
The correlations between the clinicopathologic findings and the phenotypic marker expression pattern of the tumors of 343 gastric carcinoma patients are shown in Table 3. G-phenotype tumors were associated with a lower male-to-female ratio than GI-, I-, and N-phenotype tumors (p=0.066, p=0.010, and p=0.017, respectively). N-phenotype tumors were associated with more corporeal location than were GI- and I-phenotype tumors (p=0.009 and p=0.007, respectively), a larger size than I-phenotype tumors (p=0.007), a higher proportion of advanced gastric cancers than G-, GI-, and I-phenotype tumors (p=0.003, p<0.001, and p<0.001, respectively), more perineural invasion than G-, GI-, and I-phenotype tumors (p=0.076, p=0.003, and p=0.003, respectively), and more lymph node metastasis than GI-phenotype tumors (p=0.017). I-phenotype tumors were associated with a higher proportion of intestinal-type tumors than G-, GI-, and N-phenotype tumors (p<0.001, p=0.011, and p<0.001, respectively).
DISCUSSION
In the present study, 343 gastric carcinomas were classified as G-phenotype tumors (114; 33.2%), GI-phenotype tumors (88; 25.7%), I-phenotype tumors (92; 26.8%), and N-phenotype tumors (49; 14.3%). Previous reports have shown the incidences of G-, GI-, I-, and N-phenotype tumors to be 17.7~41.1%, 20.3~60.1%, 18.5~46.6%, and 0~31.6%, respectively10, 15, 22, 26, 27). These data are consistent with our results. These results indicate that gastric carcinomas can express both the G-phenotype and the I-phenotype to varying degrees.
Here, we showed the expression of MUC5AC, MUC2C, and CD10 demonstrated in 182 (53.1%), 157 (45.8%), and 61 (17.8%) of the 343 gastric carcinomas, results which are compatible with previous studies10, 19, 22, 28). The MUC6 expression (60/343, 17.5%) in the present study differed from the results of the study by Tajima et al.10), who found MUC6 expression in 87 (64%) of 136 gastric carcinomas. However, our data was in agreement with several other reports which found that MUC6 immuno-expression was present in about 13~37% of gastric cancers, and these previous reports demonstrated this using the same anti-MUC6 monoclonal antibody19,22, 25, 28, 29). Therefore, we must consider the possibility that the rate for MUC6 expression might be linked with the predomination of the G- and GI-phenotypes (36.8% and 41.2%, respectively), and the consequent lower proportion of I- and N-phenotypes (15.4% and 6.6%, respectively), as reported by Tajima et al.10). In regards to the correlations between the clinicopathologic findings and MUC2 expression, some reports have shown no significant correlation between the two10, 28, 30). However, Utsunomiya et al.31) reported that MUC2 expression by the tumor was associated with lower levels of invasion and lymph node metastasis. We also found that MUC2 expression was associated with early gastric carcinoma and a lower proportion of lymph node metastasis. The reason for the discrepancies between the results of the aforementioned study and our results may be that the patients in most of the previous studies had advanced gastric carcinoma, whereas our study, and that of Utsunomiya et al., consisted of patients with both early and advanced gastric carcinoma. Additionally, we found that MUC2 expression correlated with a higher proportion of antral location and intestinal-type tumors, and a lower proportion of perineural invasion. In regards to the correlations between the clinicopathologic findings and CD10 expression, CD10 expression was reported to be correlated with a higher rate of differentiated-type tumors10, 32) and a higher male-to-female ratio10). We also found that CD10 expression was associated with a higher male-to-female ratio, a higher proportion of intestinal-type tumors, and a higher mean patient age.
MUC5AC expression was previously reported to have no association with any clinicopathological features19, 20). It was, however, reported to have an association with early gastric carcinoma33) and diffuse-type carcinoma28, 33). In the present study, MUC5AC expression correlated with a higher proportion of diffuse-type tumors and a lower male-to-female ratio. MUC6 expression was previously reported to have no association with any clinicopathologic features10, 19, 28). We also found no correlations between MUC6 expression and any of the variables examined.
In the previous studies, no correlation was reported between the phenotypic marker expression pattern of the tumor and gender9, 10, 22). Yet, in the present study, G-phenotype tumors were associated with a lower male-to-female ratio than the other types of tumor. Tajima et al.10) reported that I-phenotype tumors were associated with a higher rate of differentiated-type tumors than G-phenotype tumors. Similarly, in the present study, the I-phenotype tumors were associated with a higher proportion of intestinal-type tumors than G-, GI-, and N-phenotype tumors. Tajima et al.10) have previously shown that G-phenotype tumors were associated with a significantly poorer outcome than I-phenotype tumors. Mizoshita et al.22) reported that the 5-year survival rates forpatients with G-, GI-, I-, and N-phenotype gastric cancers were 37.5%, 72.2%, 54.7%, and 33.9%, respectively. They also showed that patients with GI-phenotype cancers had the best outcome and those with N-phenotype had the worst outcome. Additionally, they reported that the phenotypic classification was an independent prognostic factor, together with depth of invasion and lymph node metastasis. Our results similarly showed that N-phenotype tumors were associated with a higher proportion of advanced gastric cancers and a higher proportion of perineural invasion than tumors of other phenotypes. Moreover, N-phenotype tumors were also associated with more lymph node metastasis than GI-phenotype tumors. These results may be partially explained by the fact that the phenotypic expression of mucin may have changed during the course of the disease, especially in the case of larger tumors. These later-stage cancer lesions may lose the mucin phenotype that had been expressed at an earlier stage.
In conclusion, we have shown that N-phenotype tumors were associated with a higher proportion of advanced gastric cancer and a higher proportion of perineural invasion than tumors of other phenotypes. These results indicate that evaluating the phenotypic marker expression pattern, as determined by the combination of MUC5AC, MUC6, MUC2, and CD10 expression, is prognostically useful for patients with gastric carcinoma.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





