


INTRODUCTION
The prevalence of obesity has been steadily and significantly increasing worldwide [1,2]. Because of its impact on cardiovascular diseases (CVDs), obesity is becoming one of the most serious global health issues [3]. The risk factors associated with obesity and ischemic heart disease (IHD) are well-established, and obesity itself has been thought to be a risk factor for IHD and can worsen its prognosis regardless of the metabolic status [4,5]. There is less evidence showing obesity as an independent risk factor of end-stage renal disease (ESRD), regardless on the presence of type 2 diabetes mellitus (DM) [6], and observational studies have shown positive associations between obesity and chronic kidney disease (CKD) or ESRD [7,8]. However, some studies showed that obesity did not increase the risk of ESRD in patients with moderate to advanced CKD [9]. Therefore, whether obesity is associated with the development of ESRD remains unclear.
Percutaneous coronary intervention (PCI) is an essential treatment modality for coronary artery disease. Although PCI is mainly performed in patients with underlying diseases such as DM, CKD, and hypertension, resulting in ESRD, there is insufficient data on the association between PCI and ESRD. In addition, the impact of obesity prior to PCI on ESRD risk has not been evaluated.
Therefore, we conducted this study to verify the relationship between obesity prior to PCI and ESRD risk using the National Health Insurance Service (NHIS) health checkup data.
METHODS
Because of the confidentiality of the data used for this study and strict privacy policy from the data holder that the data can be kept among the designated research personnel only, the data cannot be provided to others, even if the data are made anonymous.
Study design and database
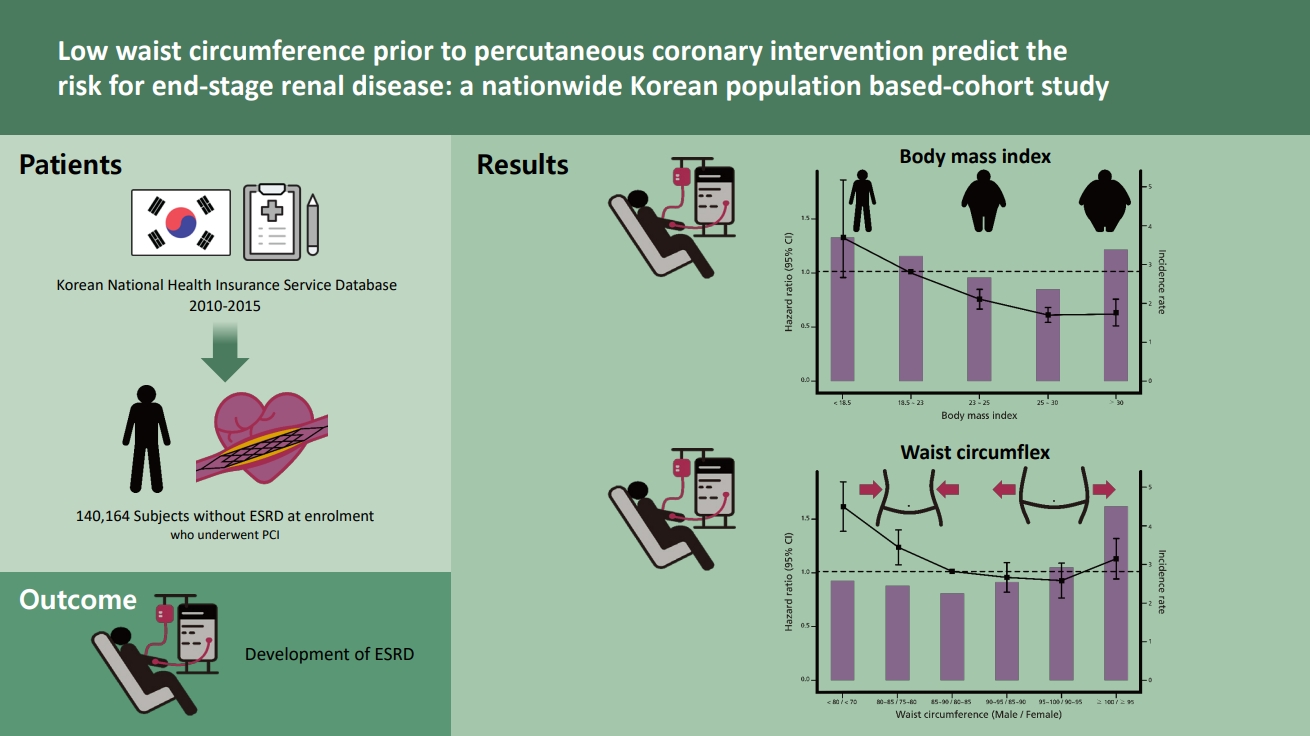
The Korean National Health Insurance Service (KNHIS) comprises a complete set of health information pertaining to 50 million Koreans, which includes an eligibility database, medical treatment database, health examination database, and medical care institution database [10,11]. The National Health Insurance Corporation (NHIC) is the single insurer, managed by the Korean government, to which approximately 97% of the Korean population subscribes. Enrollees in the NHIC are recommended to undergo a standardized medical examination at least every 2ŌĆēyears. Among 270,237 subjects who underwent PCI in 2010 to 2015 (index year), 143,727 subjects were followed up to 31 December 2017. We excluded 2,440 subjects with missing data for at least one variable. To avoid confounders by pre-existing diseases and minimize the possible effects of reverse causality, those who had a history of ESRD before the index year were also excluded (n = 1,123). Ultimately, the study population consisted of 140,164 subjects (Fig. 1). We registered only de novo PCI and excluded patients with a history of PCI to avoid the effects of past coronary intervention due to coronary artery disease, including angina pectoris or MI.
The study protocol adhered to the ethical guidelines of the 2013 Declaration of Helsinki and was approved by the Chonnam National University Hospital (study approval number: CNUH-EXP-2020-187) and NHIS (NHIS-2019-1-379). The need for written informed consent was waived by our review board.
Definitions of body mass index and waist circumference
For each participant, the body mass index (BMI) was calculated by dividing the weight (in kg) by the square of the height (in m2). We defined obesity as a BMI Ōēź 25 kg/m2. Participants were then categorized by the definition of obesity as follows: underweight (BMI < 18.5 kg/m2), normal (Ōēź 18.5 to < 23 kg/m2), overweight (Ōēź 23 to < 25 kg/m2), stage 1 obesity (Ōēź 25 to 30 kg/m2), and stage 2 obesity (Ōēź 30 kg/m2) according to the World Health Organization recommendations for Asian populations [12].
The waist circumference (WC) of each participant was also measured at the midpoint between the rib cage and iliac crest by a trained examiner. Patients were divided into six categories based on 5-cm WC increments: < 80/< 75, 80ŌĆō85/75ŌĆō80, 85ŌĆō90/80ŌĆō85 (reference group), 90ŌĆō95/85ŌĆō90, 95ŌĆō100/90ŌĆō95, and Ōēź 100/Ōēź 95 cm in men/women. Central obesity was defined as a WC Ōēź 90 cm in men and Ōēź 85 cm in women according to the definition of the Korean Society for the Study of Obesity [13].
Glycemic status and definition of chronic disease
All participants were categorized into four groups based on their glycemic status: normal, impaired fasting glucose (IFG), DM < 5 years, and DM Ōēź 5 years. IFG was defined as a facing plasma glucose level of 100 to 125 mg/dL. Type 2 DM was defined as an FPG level Ōēź 126 mg/dL or at least one claim per year for the prescription of hypoglycemic drug under International Classification of Diseases, 10th Revision (ICD-10) codes E11ŌĆō14 [14]. Patients with type 1 DM who had claims under ICD-10 code E10 were excluded from this study [15,16]. The group with DM < 5 years was defined as who had type 2 DM with 5 years on the date of the health checkup. The group with DM Ōēź 5 years was defined as those who had type 2 DM 5 years before the date of the health checkup. Comorbidities were identified using information gathered in the 1 year before the index date. Hypertension was defined as a previous hypertension diagnosis ICD-10 codes (I10ŌĆō13, I15) and a history of taking at least one antihypertensive drug, or a recorded systolic blood pressure (BP) of Ōēź 140 mmHg or diastolic BP of Ōēź 90 mmHg in the health examination database. Dyslipidemia was identified using the appropriate diagnostic code (E78) and a history of lipid-lowering drug use, or a total serum cholesterol concentration of Ōēź 240 mg/dL in the health examination database. CKD was defined as an estimated glomerular filtration rate (eGFR) of <60 mL/min/1.73 m2 calculated using Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation and as a combination of ICD-10 codes (N18ŌĆō19). ParticipantsŌĆÖ fasting blood glucose (mg/dL), total cholesterol (mg/dL), triglyceride (mg/dL), high density lipoprotein cholesterol (mg/dL), and low density lipoprotein cholesterol (mg/dL) concentrations were measured in a fasting state. The quality of the laboratory tests has been validated by the Korean Association for Laboratory Medicine, and hospitals participating in the NHI health checkup programs are certified by the NHIS.
Study outcomes and follow-up
The study population was followed from baseline to the date of ESRD diagnosis or until 31 December 2017, whichever came first. The primary end point was incident ESRD, which was defined using a combination of ICD-10 codes (Z49, Z94.0, and Z99.2) and a special code (V code) that was assigned in the initiation of renal replacement therapy (hemodialysis [HD], V001; peritoneal dialysis [PD], V003) and/or kidney transplantation (KT, V005) during hospitalization. All medical expenses for dialysis are reimbursed using the Korean Health Insurance Review and Assessment Service database. These patients are also registered as special medical aid beneficiaries. Therefore, we were able to identify every patient with ESRD in the entire South Korean population and to analyze the data for all patients with ESRD who started dialysis. Codes for treatment or medical expense claims included V005 for KT, V001 for HD, and V003 for PD. We excluded individuals without previous CKD who had a transplant or dialysis code on the same date as an acute renal failure code. Subjects on continuous renal replacement therapy or acute PD were also excluded.
General health behaviors and sociodemographic variables
Smoking history was categorized as nonsmokers, former smokers, and current smokers. Alcohol drinking was categorized into 0, 1ŌĆō2, or Ōēź 3 times/week by frequency (none, mild, and heavy, respectively), and regular exercise, defined as vigorous physical activity for at least 20 min/day, was categorized into 0, 1ŌĆō4, and Ōēź 5 times/week by frequency. Income level was divided by quartile: Q1 (lowest), Q2, Q3, and Q4 (highest).
Statistical analysis
We report the mean ┬▒ standard deviation with intervals for continuous variables and the numbers (with percentages) for categorical variables. The hazard ratios (HRs) with 95% confidence intervals (CIs) for ESRD by BMI and WC category was obtained using multivariable Cox proportional hazard models using the normal BMI (BMI 18.5 to 23 kg/m2) and normal WC (85ŌĆō90/80ŌĆō85 cm) as a reference after adjustment using four models: Model 1: crude model; Model 2: adjusted for Model 1 plus age, sex, income, DM, dyslipidemia, and hypertension; Model 3: adjusted for Model 2 plus smoking, alcohol drinking, physical activity, and eGFR; and Model 4: adjusted for Model 3 plus previous CVD, heart failure, and cancer. For the Cox proportional hazard regression model, we did not subtract the deceased from the data itself to minimize possible bias when excluding mortality and morbidity.
The cumulative ESRD incidence was estimated by constructing Kaplan-Meier curves for the mean 5.4-year follow-up period, and we used the log-rank test to examine differences in ESRD development by the level of BMI and WC. We also performed subgroup analysis for DM status. A p < 0.05 was considered to reflect statistical significance. SAS version 9.3 software and SAS survey procedures (SAS Institute Inc., Cary, NC, USA) were used for all statistical analyses.
RESULTS
Baseline characteristics
Among all the participants, 2,082 (1.49%) developed ESRD during a median follow-up duration of 5.4 years. The mean age was higher among individuals who developed ESRD than among those who did not. The proportions of low income were higher in the incident ESRD than in the non-ESRD groups. Comorbidities such as DM, hypertension, dyslipidemia, CKD, proteinuria, CVD, heart failure, and cancer were more prevalent in the ESRD group than in the non-ESRD group. eGFR and BMI were lower, and BP and glucose levels were higher, in the ESRD group than in the non-ESRD group (Supplementary Table 1).
The characteristics of participants classified by BMI levels and WC are presented in Tables 1 and 2, respectively. Subjects in the underweight group (BMI < 18.5 kg/m2) were older; had a lower income; exercised less; and had a lower prevalence of DM, hypertension, dyslipidemia, and CKD, and a higher prevalence of CVD, heart failure, and cancer. The mortality rate was highest in the underweight group. BP, fasting glucose, and total cholesterol were lower in the underweight group (Table 1). Table 2 shows that the patients in the central obesity group were older; mostly women; had a lower income; exercised less; and had a higher prevalence of DM, hypertension, dyslipidemia, CKD, CVD, and heart failure. Apart from eGFR, BP, fasting glucose, and lipid levels were also higher in the central obesity group. The mortality rate was highest in the WC of < 80/< 75 (Table 2).
Association of BMI and WC with the risk of ESRD
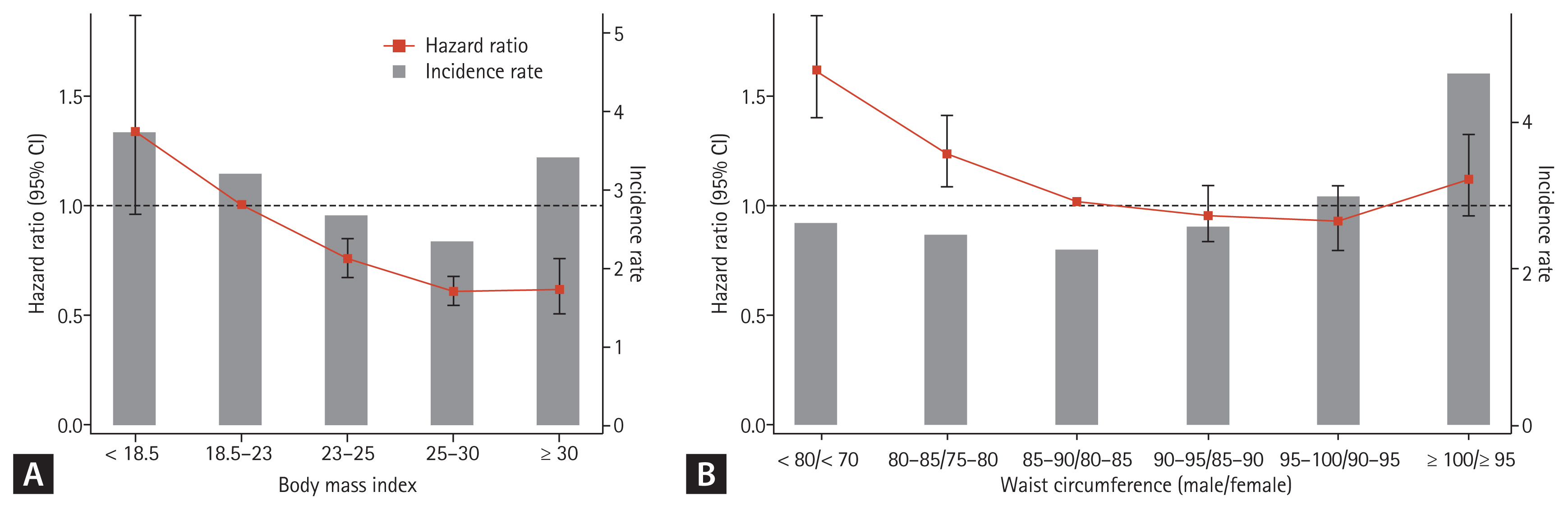
The underweight group (HR, 1.331; 95% CI, 0.955 to 1.856) and the WC < ŌłÆ80/ŌłÆ75 group (HR, 1.589; 95% CI, 1.379 to 1.831) showed the highest ESRD risk, while the BMI 25 to 30 group showed the lowest ESRD risk (HR, 0.604; 95% CI, 0.542 to 0.673) in all participants after adjusting for age, sex, income, presence of DM, dyslipidemia, hypertension, smoking, alcohol drinking, physical activity, glomerular filtration rate, previous CVD, heart failure, and cancer (Table 3 and Fig. 2). Central obesity prior to PCI tended to show a risk factor for ESRD development, but it was not statistically significant (Table 3 and Fig. 2B).
Subgroup analyses
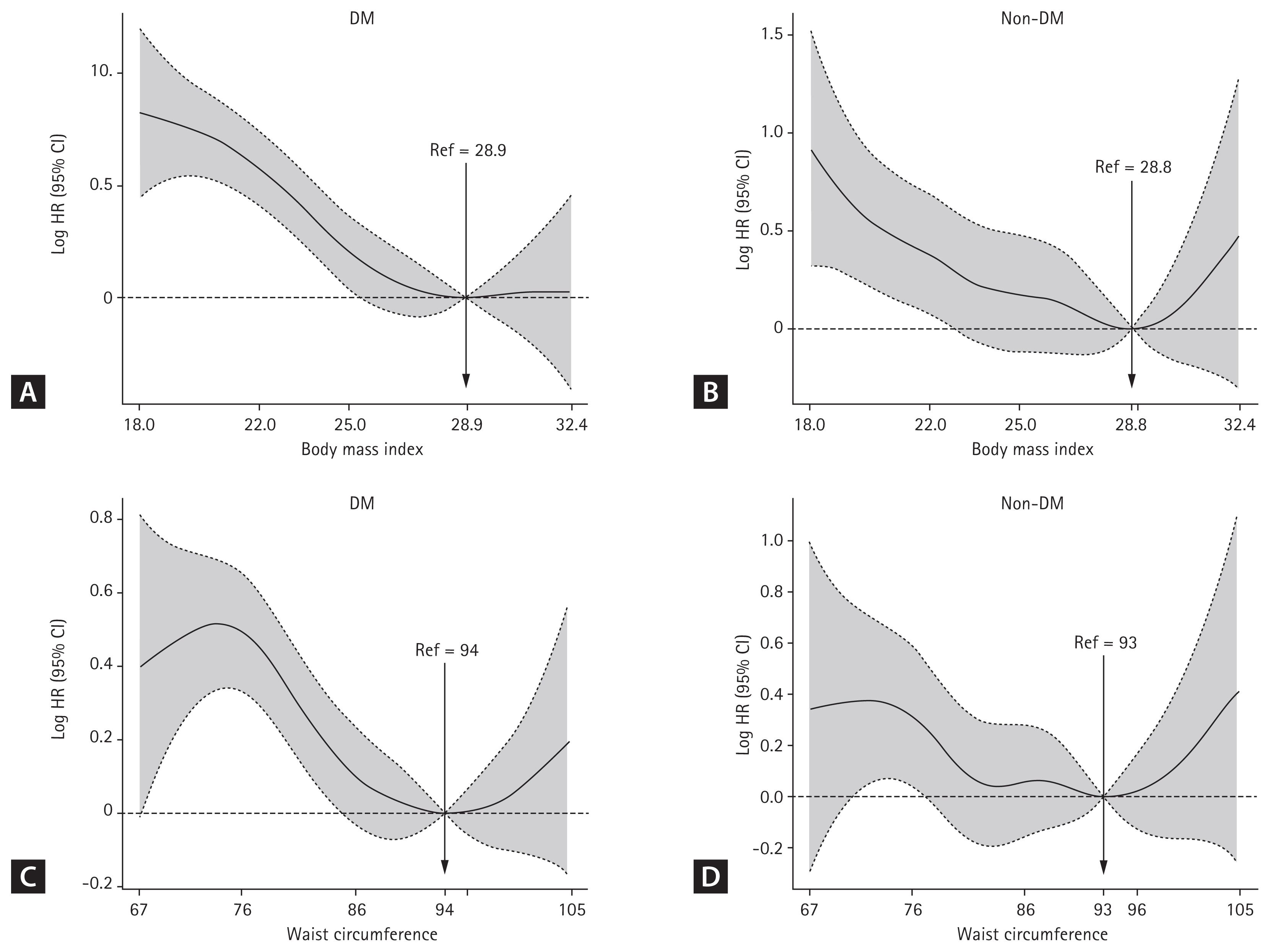
Subgroup analyses for DM and DM duration were performed. The DM group showed a reverse linear relationship with ESRD risk at BMI values below 28.9 kg/m2 (Fig. 3A) and WC values below 94 cm (Fig. 3C). However, this reverse linear relationship with ESRD risk was not statistically significant for the non-DM group (Fig. 3B and 3D).
In the DM duration subgroup analysis, the BMI level prior to PCI was not a risk factor for ESRD in all four groups after adjustment with all variables (Table 4). A WC < 85/80 cm (men/women) increased ESRD risk in only DM group (DM < 5 years and DM Ōēź 5 years) compared to the reference group (85ŌĆō90/80ŌĆō85 of WC), but not the normal or IFG groups (Table 5).
DISCUSSION
The present study demonstrated that low WC prior to PCI was associated with a higher risk of ESRD during a 5.4-year follow-up period after PCI. Moreover, this phenomenon was more obvious in the DM group than in the non-DM group. This association persisted after multivariable adjustment for important potential confounders.
Generally, BMI, an internationally accepted standard anthropomorphic measurement, is used to define obesity in research settings [17]. Several studies have examined the association between BMI and future risk of ESRD. Although the results are conflicting, most epidemiologic studies showed that a higher BMI was associated with an increased risk of kidney disease. Two large epidemiologic studies in the United States reported a positive association between BMI and ESRD, and these studies analyzed a broad spectrum of BMI among a large, diverse sample of participants with long-term follow-up for ESRD [7,8]. It is presumed that a higher BMI is an independent risk factor for ESRD in any ethnic group.
However, the association between BMI with future risk for ESRD tends to be discordant in patients with renal impairment, and this population thus exhibits a so-called ŌĆ£obesity paradox.ŌĆØ Specifically, although a high BMI is associated with all-cause mortality and decreased renal function in patients with earlier stages of CKD, this association is attenuated in patients with advanced CKD [18,19]. In addition, a few studies also showed that patients with obesity paradoxically exhibited more favorable clinical outcomes with respect to in-hospital, short-, and long-term mortality than those without obesity after PCI [20ŌĆō23]. Therefore, there are still controversies between BMI and the risk for future ESRD in PCI patients. We therefore considered that longitudinal studies are required to explore the actual relationship between BMI and the risk of ESRD. To the best our knowledge, this is the first nationwide cohort study that examines the relationship between lower BMI and ESRD risk in the Korean population prior to PCI. Our findings were inconsistent with most previous published studies, showing that BMI prior to PCI was not associated with risk for ESRD.
Recently, measures of central or abdominal obesity, defined by the WC and waist-hip ratio, have been used as more important predictors to assess the mortality risk than BMI [24,25]. WC, a representative marker of visceral body fat, was found to correlate with inflammation, whereas subcutaneous body fat may be an indicator of the nutritional status [26]. In patients with ESRD, multiple studies identified WC as a direct and strong predictor of mortality and incident cardiovascular events, even after adjusting for the BMI and other risk factors [27,28]. In fact, many studies have shown that central obesity or abdominal adiposity measured by the WC was linearly associated with a higher risk of mortality after PCI [29]. However, our findings show that a WC under < ŌłÆ80/< ŌłÆ75 cm showed the highest risk for future ESRD development as well as higher mortality. Increasing WC was also linearly associated with a lower risk of future ESRD development. However, unlike BMI, low WC prior to PCI was a risk for ESRD, especially in the DM group, suggesting that WC maybe more accurate than BMI to estimate the risk for ESRD in prior to PCI. In our study, there was tendency of a WC of Ōēź 100/Ōēź 95 cm (men/women) to increase the risk of ESRD in the DM and non-DM groups. More research on central obesity as a risk factor is needed.
The exact mechanisms by which a low WC presents a high risk for ESRD development in PCI patients are not known. High adiposity itself has been reported as a predictor of good prognosis among patients with coronary artery disease. Lavie et al. [30] reported that a high percentage of body fat, which was measured using the sum of the skinfold method, was associated with a low mortality rate among patients with stable angina. However, more systematic studies are needed to confirm this hypothesis.
Our study has several limitations. First, we did not collect relevant information on the food habits or other comorbidities that might affect weight. Second, this study did not consider use of medications such as hypoglycemic agents or lipid lowing agents, and adherence to treatment. Third, we were unable to obtain more information about the causes of ESRD. Fourth, we used data from the NHIS checkup program in a Korean population; therefore, we cannot generalize the results to other ethnic groups. Fifth, although we monitored the subjects for 5.4 years, the time of follow-up is short for patients to develop ESRD. Sixth, because of the nature of the claim data, we were unable to evaluate the indication or purpose of the PCI.
In conclusion, to the best of our knowledge, this is the first study on the relationship between BMI and WC prior to PCI and ESRD development in a large general population using a well-established and validated longitudinal national database for around 5.4 years. Our study demonstrated that low WC prior to PCI, which showed the increased ESRD risk in patients undergoing PCI, especially in those with DM.
KEY MESSAGE
1. This is the first study on the relationship between body mass index (BMI) and waist circumference (WC) prior to percutaneous coronary intervention (PCI) and end-stage renal disease (ESRD) development.
2. The BMI prior to PCI was not a risk factor for ESRD with or without diabetes mellitus (DM).
3. Low WC prior to PCI showed an increased ESRD risk in patients undergoing PCI, especially in those with DM.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





