


INTRODUCTION
Cardiovascular disease (CVD) is becoming more prevalent worldwide and is one of the leading causes of death [1]. To lower CVD mortality, aggressive and comprehensive management of its risk factors, including dyslipidemia, hypertension, diabetes mellitus, and smoking, are crucial [2]. The incidence of coronary artery disease (CAD) is rising in South Korea and although cerebral hemorrhage has declined since 2002, cerebral infarction is on the rise [3]. This is speculated to be due to the elevated prevalence of dyslipidemia and diabetes mellitus with the growing obesity population, while hypertension is well-managed and smoking rate has reached a plateau [4]. Thus, aggressive diagnosis and treatment of dyslipidemia, the most important risk factor for atherosclerosis, are critical for lowering the incidence and mortality of CAD and cerebral infarction.
To promote appropriate treatment of dyslipidemia, the Korean Society of Lipid and Atherosclerosis (KSo-LA) published the first guidelines for the management of hyperlipidemia in 1996, the second guideline in 2003, the second revision in 2009, and the third guidelines for treatment of dyslipidemia with added contents in 2015, in collaboration with 18 other relevant academic societies and organizations [5]. However, new guidelines were published in Europe in 2016 and in the United States in 2017 based on new study findings, and new drugs, such as proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have been launched [6-8]. Therefore, the KSoLA Treatment Guideline Committee developed the fourth guidelines for treatment and management of dyslipidemia specific to Koreans based on evidence and expert opinions on the dynamically changing treatment modalities for dyslipidemia.
The fourth guideline consists of information about the epidemiology of dyslipidemia, diagnosis and treatment criteria, lifestyle interventions, drug therapy, and dyslipidemia in specific patient groups. Finally, we present currently available data and the need to develop and validate scales to assess the risk of CVD specific to Koreans and CVD biomarkers appropriate for the Korean population. The level of evidence and strength of recommendations used in the fourth guideline are shown in Table 1. The fourth guideline is available in full text and an abstract form including tables and figures in Korean. This paper is an English summary of the full text. We hope the fourth guidelines for the treatment of dyslipidemia will be useful for health professionals treating dyslipidemia.
EPIDEMIOLOGY OF DYSLIPIDEMIA IN KOREANS
Cardiovascular disease in Koreans
CVD is the leading cause of deaths worldwide, with an estimated 17 million people dying from CVD every year [1,2]. In South Korea, the death rate resulting from diseases of the circulatory system was 187 men per 100,000 population and 145 women per 100,000 population in 1983 and 111 men per 100,000 population and 125 women per 100,000 in 2016, indicating little change over the years. However, the age-adjusted mortality rate, which excludes the influence of aging of the population during this period, decreased to about one-fifth of the initial rate (Fig. 1). Death from CAD has consistently increased since 1983, when the cause of death statistics were first measured, reaching 31 men per 100,000 and 26 women per 100,000 in 2016. However, age-adjusted mortality of CAD reached a peak in the early and mid-2000s and began to decline since then (Fig. 2). Deaths from cerebrovascular disease declined since 2000s, reaching 44 men per 100,000 and 47 women per 100,000 in 2016. Age-adjusted mortality for cerebrovascular disease has declined very quickly (Fig. 3). Among various cerebrovascular diseases, there were more deaths from cerebral hemorrhage (non-traumatic intracerebral hemorrhage and subarachnoid hemorrhage) until 2002, but deaths from cerebral infarction (ischemic stroke) have become more common since then. This is speculated to be due to the marked decline in the incidence and improved treatment outcomes of cerebral hemorrhage as a result of advances in treatment for hypertension [9].
The prevalence and incidence of CVD are not accurately known due to a lack of nationwide statistics. Based on a review of various studies, however, the prevalence of CVD is rising and the trend of incidence is predicted to vary according to the type of disease. Recent studies using health insurance claims data have reported the incidence of acute myocardial infarction (MI) to be about 50 and 10 per 100,000 for men and women, respectively [4,5,9]. For cerebrovascular disease, the incidence of cerebral infraction and cerebral hemorrhage differs, where cerebral hemorrhage is declining quickly while cerebral infarction is slowly rising, eventually resulting in the number of cases of cerebral infraction outnumbering those of cerebral hemorrhage. It is generally believed that the incidence of CVD differs across regions and over time due to the changing distribution of CVD risk factors [10]. The prevalence of hypertension in South Korea is largely consistent with the smoking rate reaching a lower plateau; however, the prevalence of diabetes mellitus and dyslipidemia is on the rise. Thus, it is predicted that CAD would become the most prevalent CVD in Korea [11,12].
CVD risk factors and risk assessment for Koreans
The risk factors for CVD are well known, and the incidence of CVD varies across regions and time paralleling the distribution of these CVD risk factors across regions and time [10]. Among CVD risk factors, those that have a significant impact on the disease but are able to be treated are referred to as major modifiable risk factors and include hypertension, diabetes, dyslipidemia, and smoking [12]. Other CVD risk factors include family history, old age, lack of exercise, obesity, chronic inflammation, blood coagulation abnormalities, metabolic syndrome, depression, and stress. A Korean cohort study that analyzed the population attributable risk found that the contribution is the highest for hypertension, followed by smoking, dyslipidemia, and diabetes in men; the contribution by all four risk factors reaches 64%. In Korean women, the factor with the highest contribution to CVD risk was hypertension, followed by dyslipidemia, diabetes, and smoking (Table 1) [13]. Recently, many studies have attempted to assess CVD risk based on a comprehensive review of exposure to various CVD risk factors [14]. Since the development of the Framingham risk score by the Framingham Heart Study to compute the 10-year risk of CAD using seven items of information (age, sex, total cholesterol, high density lipoprotein cholesterol [HDL-C], blood pressure, diabetes, and smoking), various CVD prediction models have been developed, and a CVD prediction recommendation guideline has been formulated. In South Korea, there are studies available that developed a stroke risk model, a CAD risk model, and a CVD risk assessment model using data from health check-up recipients [13,15-19].
Distribution of lipid concentration in Koreans
The distribution of serum lipid concentrations varies according to sex and age and there is a notable difference among women before and after menopause. Total blood cholesterol concentration was reported to slightly decrease in the 15- to 19-year-old age group compared to that in the 10- to 14-year-old group, but increase again after the age of 20 years in both sexes [20]. In the teen years, total cholesterol is higher among women. In individuals in their thirties and forties, total cholesterol is higher among men, but women actually have a higher total cholesterol concentration after the mid-50s (Fig. 4A). Distribution of low density lipoprotein cholesterol (LDL-C) concentration is similar to that of total cholesterol (Fig. 4B) [20]. Triglyceride concentration on rapidly increases from the age of 10 to 40 years, is maintained at a high level between ages 40 to 60, and gradually decreases after the age of 60 in men. Conversely, in women, triglyceride concentration is very low until the ages of 30 to 40, begins to increase after the mid-40s, and peaks after the age of 65 (Fig. 4C) [20]. HDL-C concentration is higher among women than men in across all age groups, and the gap is greater in the 20- to 30-year-old group (Fig. 4D) [20].
The prevalence of hypercholesterolemia in adults aged 30 years or older in South Korea (total cholesterol ≥ 240 mg/dL or on cholesterol-lowering drugs) has risen consistently, from 7% and 8% in men and women, respectively, in 2005, to 19% and 20%, respectively, in 2016 (Fig. 5A) [21]. The prevalence of dyslipidemia was more than double that of hypercholesterolemia at 40.5%. Sexand age-differences indicate that the prevalence of dyslipidemia in men is the highest between the ages of 55 to 59 years (49%) and gradually declines thereafter, while prevalence in women is low between the ages of 20 to 44 years, after which it rapidly increases to 50% between the ages of 60 to 64 years, eventually exceeding that of male counterparts (Fig. 5B) [22]. The prevalence of dyslipidemia is higher among individuals with other comorbidities, such as obesity, abdominal obesity, and diabetes than among those with no comorbidities [23].
Fortunately, indices for management, such as hypercholesterolemia awareness rate, treatment rate, and control rates, have been improving. The hypercholesterolemia awareness rate (the percentage of individuals diagnosed among all those who have hypercholesterolemia) increased from 24% in 2005 to 58% in 2016. In the same period, the treatment rate (the percentage of patients taking cholesterol-lowering drugs) increased from 17% to 49%, the patient control rate (the percentage of patients with total cholesterol < 200 mg/dL) increased from 11% to 41%, and the treated patients control rate (the percentage of treated patients with total cholesterol < 200 mg/dL) increased from 62% to 83% (Fig. 6) [21]. These management indices have improved in both men and women overall, but the awareness rate and treatment rates have remained low at about 20% to 30% among those below age 50 even until recently (Table 2) [21].
DIAGNOSIS AND TREATMENT CRITERIA FOR DYSLIPIDEMIA
Recommendation
Diagnostic approach and criteria
Dyslipidemia is generally asymptomatic, so a screening test is essential to identify patients requiring treatment. For screening of dyslipidemia, all adults aged ≥ 21 years and younger individuals with other risk factors, such as a family history of premature CVD and severe dyslipidemia, should undergo a fasting lipid test every 4 to 6 years to assess total cholesterol, triglyceride, HDL-C, LDL-C (calculated using the Friedewald equation or perform a direct assay when triglyceride level is ≤ 400 mg/dL), and non-HDL-C levels [6,24].
For the measurement of triglyceride and LDL-C levels, individuals must fast for at least 12 hours before blood sampling. LDL-C concentration can be generally estimated from fasting total cholesterol, triglyceride, and HDL-C. That is, if the individual’s triglyceride concentration is ≤ 400 mg/dL, very low density lipoprotein cholesterol (VLDL-C) concentration can be estimated by dividing the triglyceride value by 5. As total cholesterol is the sum of LDL-C, HDL-C, and VLDL-C concentrations, LDL-C concentration can be calculated using the Friedewald equation below:
However, if the individual’s triglyceride concentration > 400 mg/dL, the LDL-C value estimated from the above equation is less accurate. In such cases, we recommend using the LDL-C direct assay [25]. In addition, the cause of hypertriglyceridemia should be further investigated.
Treatment guideline
In this treatment guideline, we maintained the existing system of differentiating target LDL-C concentration based on the level of CVD risk factors, as previously used in the current treatment guideline in Korea, but modified and supplemented the specific risk factors and treatment standards with reference to study findings in Korea and abroad as well as with the 2013 American College of Cardiology (ACC)/American Heart Association (AHA), 2016 European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS), and treatment guidelines published in other countries [6]. One benefit of the 2013 ACC/AHA treatment guideline is that it simplified the criteria for statin administration to “four statin benefit groups,” but it has been reported that the practical application of the criteria would be difficult due to several problems [21]. Therefore, we did not deviate significantly from the third revision of Korean dyslipidemia guidelines.
Very high-risk group
Patients with CVD (CAD, peripheral artery disease, ischemic stroke, transient ischemic attack) are classified as the very high-risk group. For this group, the goal should be set to lowering LDL-C to < 70 mg/dL or by more than 50% of the baseline level for secondary prevention. Furthermore, when acute MI occurs, statin should be immediately administered regardless of the baseline LDL-C concentration (Tables 3 and 4).
In a foreign randomized trial to test low-dose or highdose statin administration on 10,000 patients with stable angina with LDL-C < 130 mg/dL, lowering LDL-C level close to 70 mg/dL with high-dose statin administration reduced CVD risk by about 22% [26]. Furthermore, a meta-analysis of patients who received statin reported that preventive effects against CVD were the greatest when LDL-C was reduced to a level < 70 mg/dL or by > 50% of the baseline level [27].
The 2018 AACE/ACE guidelines recommend that patients with atherosclerotic CVD and (1) atherosclerotic CVD continuing to progress even after lowering LDL-C to < 70 mg/dL, (2) diabetes, (3) stage 3 or 4 chronic kidney disease, (4) heterozygous familial hypercholesterolemia (heFH), or (5) history of premature atherosclerotic CVD (men < 55 years, women < 65 years) should be classified into the extreme risk group and that the target for LDL-C should be set to < 55 mg/dL [28]. This recommendation stems from the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), which proved the superiority of combined statin and ezetimibe therapy for patients with acute coronary artery syndrome, and the Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER) study and the ODYSSEY OUTCOMES trial, which confirmed the effects of PCSK9 inhibitors [29-31]. These three studies documented that lowering the targeted LDL-C concentration to below the previous target is additionally beneficial for prevention of major CVD events particularly for the extreme risk group. These findings suggest that it may be necessary to lower the LDL-C target level for patients with clinical apparent atherosclerotic CVD (particularly acute coronary artery syndrome). However, additional studies are needed to investigate cost-effectiveness and application in Korean patients.
Furthermore, a foreign randomized trial on 4,700 patients who experienced ischemic stroke or transient ischemic attack within 6 months found that the LDL-C concentration was 73 mg/dL in the statin group and 129 mg/dL in the placebo group and that the risks of stroke and CVD significantly decreased by 16% and 20%, respectively, in the statin group, which suggested that lowering LDL-C to close to 70 mg/dL through statin administration would also be helpful for patients who had an ischemic stroke [32]. However, considering that the Korea Medical Insurance Corporation (KMIC) study and Japan’s National Integrated Project for Prospective Observation of Non-communicable Disease and its Trends in the Aged (NIPPON DATA80) cohort study reported that hypertension, as opposed to hypercholesterolemia, was more strongly associated with cerebrovascular diseases and that high-dose statin administration reduced the incidence of ischemic stroke but increased that of hemorrhagic stroke, additional Korean studies are needed to further investigate the statin dose and LDL-C targets for preventing ischemic stroke [33].
When acute MI occurs, it is recommended to administer statins immediately regardless of the baseline LDL-C level. In a randomized controlled trial (RCT) on 4,500 patients who experienced an acute MI, the incidence of CVD was lower in the group that received statin immediately after MI than in the group that did not receive statin immediately after MI [34]. In a Korean study, though a retrospective follow-up using registry, of about 1,000 patients whose LDL-C concentration was < 70 mg/dL at the time of MI, the 1-year incidence of CVD was lower in the group that immediately received statin than in the group that did not [35]. Thus, in light of Korean and foreign study findings, it is recommended to administer statin immediately after acute MI regardless of the baseline LDL-C concentration.
High-risk group
Patients with carotid disease (significant carotid artery stenosis), abdominal aortic aneurysm, or diabetes are classified as a high-risk group. For this group, treatment is started when LDL-C concentration is ≥ 100 mg/dL for primary prevention [36,37]. Furthermore, for diabetes patients with target organ damage or major CVD risk factors, the target could be lowered depending on the case (Tables 3 and 4).
In the North American Symptomatic Carotid Endarterectomy Trial (NASCET) that followed-up 1,415 patients who underwent carotid endarterectomy due to carotid artery stenosis, the risk of stroke on the ipsilateral side over a period of 8 years was 17.1% higher among patients with a carotid disease [38]. Similarly, the European Carotid Surgery Trial (ECST) study showed that patients with symptomatic carotid artery stenosis had a higher cardiovascular mortality rate, with a 6-year mortality of 27% regardless of the degree of stenosis, and the 10-year cardiovascular mortality was estimated to be 30% [39,40]. In addition, many studies reported that among patients with carotid artery stenosis without CVD, lowering LDL-C by administering statin reduced major cardiovascular events and mortality [41]. Korean treatment guidelines also classified patients with carotid artery stenosis as the high-risk group but did not indicate a specific degree of stenosis.
Moderate-risk group
In line with existing Korean treatment guidelines, patients with two or more major risk factors other than LDL-C are classified into the moderate-risk group. Statin is administered if LDL-C concentration remains > 130 mg/dL even after weeks or months of lifestyle adjustment (Tables 3-5). The major risk factors listed in the Adult Treatment Panel (ATP) III and Korean guidelines were used. Among these, smoking, hypertension, age, sex, and low HDL-C have also been adopted by other treatment guidelines, including the 2013 ACC/AHA, ESC/EAS, and Japan Atherosclerosis Society (JAS) [6,24,42]. However, assessing risk based on these major risk factors is known to predict only about half of the actual cardiovascular risk; thus, individualized treatment goals should be set in consideration of other risk factors, such as obesity, physical activity, diet, levels of triglycerides, high sensitivity C-reactive protein (hs-CRP), lipoprotein(a), apolipoprotein, fibrinogen, homocysteine, and apolipoprotein B, as well as the ankle-brachial blood pressure index, carotid intimal medial thickening (< 50% stenosis but with evidence of clinical progression or accompanied by atherosclerotic plaque), and coronary calcium score [6,40].
Low-risk group
Patients with one or fewer major risk factor other than LDL-C are classified as the low-risk group. In line with previous treatment guidelines, statin is administered if LDL-C remains > 160 mg/dL even after weeks or months of lifestyle adjustment (Table 3). In the revised guideline, LDL-C target was set to < 160 mg/dL, but as other non-major risk factors were taken into consideration for the moderate-risk group, more aggressive treatment goals could be also set for the low-risk group depending on the case [40]. If LDL-C concentration is > 190 mg/dL, other causes of dyslipidemia, such as biliary obstruction, nephrotic syndrome, hypothyroidism, pregnancy, and use of glucocorticoids or a cyclosporine, should be investigated and corrected. If LDL-C concentration is > 190 mg/dL in absence of secondary causes, statin should be started irrespective of the level of risk.
Treatment guidelines for hypertriglyceridemia
The risk of acute pancreatitis is known to increase when blood triglyceride level exceeds 500 mg/dL, and in such cases, it is important to investigate secondary causes that may elevate triglyceride concentration, such as weight gain, drinking, carbohydrate intake, chronic kidney failure, diabetes, hypothyroidism, pregnancy, and use of estrogen, tamoxifen, and glucocorticoids, as well as genetic factors that may cause abnormal lipid metabolism [24,43]. If triglyceride concentration remains ≥ 500 mg/dL even in the absence or correction of secondary causes, it is recommended to begin fibrate or omega-3 fatty acid therapy to prevent pancreatitis. Further, statin should be administered if triglyceride level is between 200 to 499 mg/dL with a high LDL-C level so as to primarily lower the LDL-C concentration to the targeted level. If hypertriglyceridemia persists (≥ 200 mg/dL) even after lifestyle adjustment and statin administration in the very high-risk and high-risk groups, drugs that lower triglyceride concentration, such as fibrate and omega-3 fatty acid, can additionally be used to prevent CVD.
Statin, as opposed to other effective triglyceride-lowering drugs, such as fibrates, is recommended as the primary drug for patients with hypertriglyceridemia based on the multiple study findings indicating that statin administration is helpful for preventing CVD [44]. Whether fibrate administration is effective in preventing CVD remains controversial. In a meta-analysis of RCTs to investigate the effects of medications for dyslipidemia on mortality, statin significantly decreased cardiovascular mortality, while fibrate did not significantly lower mortality compared to placebo [45]. Considering that there have been no study findings suggesting that fibrate has superior effects to statin on preventing CVD in patients with hypertriglyceridemia, it would be appropriate to primarily administer statin in order to prevent CVD caused by hypertriglyceridemia.
Moreover, whether administration of fibrate or omega-3 fatty acid in addition to statin for patients with persistent hypertriglyceridemia even after lifestyle adjustment and statin administration lowers CVD risk is still a matter of debate. The Action to Control Cardiovascular Risk in Diabetes Action to Control Cardiovascular Risk in Diabetes (ACCORD) study reported that additional fibrate administration to about 5,500 patients with type 2 diabetes taking statin did not lower CVD or mortality. However, the same study found that pre-administration triglyceride concentration was low (162 mg/dL) in all patients and an additional analysis showed that among patients with pre-treatment triglyceride concentration ≥ 204 mg/dL with low HDL-C (≥ 34 mg/dL), the incidence of CVD differed between the fibrate (12%) and placebo (17%) groups [46]. Therefore, adding triglyceride-lowering drugs, such as fibrate and omega-3 fatty acid, to the statin regimen is recommended for high-risk patients with persistent hypertriglyceridemia (≥ 200 mg/dL) even after lifestyle adjustment and statin administration to prevent CVD.
Follow-up monitoring
In line with previous Korean guidelines and foreign guidelines, the present revision also recommends lipid testing prior to administration and another round of testing 4 to 12 weeks after beginning administration to assess response and compliance, after which it is recommended to perform lipid tests at 3- to 12-month intervals depending on the patient’s cardiovascular risk and degree of lipid reduction after drug administration. The revised guideline recommends performing a liver function test in addition to a lipid test.
In line with the existing guideline, the present revision also recommends termination of drug administration if patient develops myopathy symptoms and creatine kinase (CK) levels increase more than 10-fold. In Korea, blood creatinine levels should be measured before fibrate administration and after 3 months of administration and patients should be followed-up every 6 months if there are no other abnormal findings.
The 2013 ACC/AHA treatment guidelines could not be directly applied in Korea, as it did not reflect individual differences in drug responses by uniformly recommending a moderate-to-high dose of statin for all patients without a specific LDL-C target level, did not clearly examine the benefits and adverse reactions of high-dose statin administration, and may overestimate CVD risk in Korea. Additional studies are needed on the Korean population to set an appropriate statin dose and LDL-C target and specific goals for controlling risk factors and hypertriglyceridemia, which serve as the criteria for primary prevention.
LIFESTYLE INTERVENTIONS FOR DYSLIPIDEMIA
Diet therapy: recommendation
Energy
Obesity and overweight are related to dyslipidemia. Many studies with obese or overweight individuals found that total cholesterol, LDL-C, and triglyceride concentrations decreased with weight loss [47]. Therefore, Energy intake should be appropriate to maintain healthy weight. According WHO criteria, body mass index (BMI) of ≥ 30 kg/m2 is classified as obesity. However BMI of ≥ 25 kg/m2 proposed as obesity in Korea [48]. Obese people can expect to improve blood cholesterol and triglyceride levels even by losing about 5% to 10% of current weight. In general, a low-calorie diet that is about 500 kcal less than one’s usual intake has no particular harm to health and is reasonable to adhere to.
Fat
Traditionally, it was recommended to limit fat intake to treat dyslipidemia. Several studies have reported that limiting fat intake improves LDL-C levels, but in most cases, it is difficult to conclude that such improvement is an outcome of limiting total fat intake, as an interaction of multiple factors, such as weight loss and reducing saturated fats and trans fats, are involved. Moreover, when fat intake is limited, carbohydrate intake relatively increases, which in turn increases blood triglyceride level [49]. However, an excessively high-fat diet may have an adverse impact on blood lipid levels by increasing saturated fat and energy intake, so an appropriate amount of fat should be consumed. The 2016 ESC/EAS guideline recommends individualized rules of percent fat intake but to take precaution so as not to exceed 35% of total energy consumption, as it may result in elevated saturated fat and energy intake [6]. The average fat intake in Korean is about 20%. In Dietary Reference Intake (DRI) for Koreans 2015, 15% to 30% fat intake is recommended [50,51]. However, considering that percent fat intake varies widely across individuals and fat intake has been on the rise recently, individuals should take precaution so as not to consume fats excessively. Overall, fat intake should be limited to within 30% of total energy consumption.
The type of fatty acids has a greater impact on blood lipid levels than total fat amount. Replacing saturated fats to unsaturated fats could lower blood LDL-C level, and substituting trans fats to unsaturated fats contributes to improving blood triglyceride and HDL-C levels [52]. The 2016 ESC/EAS guideline recommends to limit saturated fats intake to < 7% of total energy intake and to limit trans fat intake to < 1% of total energy intake by avoiding processed foods [6]. The 2013 AHA/ACC guideline recommends to limit saturated fatty acid intake to 5% to 6% of total energy intake and to avoid trans fat intake [50]. Some rich sources of saturated fats include fats of meats, skin of poultry, butter, and palm oil. The major sources of trans fats are hydrogenated oils, such as margarine and shortening, and trans fats are produced during heating oil in high temperature.
N-3 fatty acids do not have a positive effect on blood cholesterol levels but 2 to 4 g of n-3 fatty acids may help lower triglyceride level for those with hypertriglyceridemia [54]. Although substituting saturated fat with polyunsaturated fat is effective in improving blood lipid levels, it is recommended to limit n-6 fatty acid intake to 10% of total energy intake.
Cholesterol intake has a less of an impact on blood LDL-C levels than saturated fats and trans fats and the effect varies widely across individuals. Due to insufficient evidence dietary cholesterol restriction in order to prevent serum LDL-C recommendation of dietary cholesterol was excluded from the 2015 Dietary Guideline for Americans. The 2013 AHA/ACC guideline does not include a recommendation about cholesterol intake [53]. The 2016 ESC/EAS guideline recommends cholesterol intake be limited to 300 mg only for individuals with high serum cholesterol level [6]. In DRI for Koreans 2015, it is recommended to reduce dietary cholesterol less than 300 mg [51]. In this context, cholesterol intake need not be limited uniformly for the prevention of dyslipidemia, but excessive intake should be avoided for individuals with hypercholesterolemia.
Carbohydrates
Excessive carbohydrate intake, particularly simple sugar intake, elevates blood triglyceride level. In Western countries, recommendation on carbohydrate restriction is not separately specified, the proportion of carbohydrate intake is not high in general population. Instead, recommendations suggest simple sugar intake to be limited and to eat fiber-rich food sources of carbohydrates. Conversely, carbohydrate is a major portion of Koreans’ diet, so Koreans should take precautions so as not to consume carbohydrates excessively. It is recommended that the total carbohydrate consumption be limited to 65% of daily energy intake, which is the upper limit of DRI for Koreans 2015 and simple sugars should be limited to 10% to 20% of daily energy intake [51].
Soluble fibers are beneficial in lowering blood cholesterol and triglyceride concentrations, and they are found in rich amounts in whole grains, seaweeds, and vegetables. The 2016 ESC/EAS guideline recommends people to consume 5 to 15 g of soluble fibers (25 to 40 g of total dietary fiber) [6,55,56]. It is recommended that people eat fiber-rich foods to ingest > 25 g of dietary fiber.
Alcohol
Excessive alcohol consumption (≥ 10 to 30 g/daily) should be avoided, as it increases blood triglyceride levels [57]. Hypertriglyceridemia due to alcohol consumption is associated with suppression of chylomicron degradation as a result of reduced lipoprotein lipase (LPL) activity. The 2016 ESC/EAS guideline recommends people to avoid heavy drinking (< 20 to 30 g for men, < 10 to 20 g for women) and to avoid drinking for patients with hypertriglyceridemia [6]. Regardless of the type of alcohol, daily drinking should be limited to one to two drinks.
Dietary pattern
Recent dietary guidelines for CVD tend to emphasize the quality of overall diets, rather than focusing on individual nutrients. These changes are based on the accumulating evidence that quality of fat intake is more important than quantity of fat intake Studies of dietary patterns for the Western population such as Dietary Approaches to Stop Hypertension (DASH) or Mediterranean dietary patterns reported the effects of dietary patterns on blood lipid levels. Based on these results, the ACC/AHA guidelines adopt dietary patterns such as the DASH, the United States Department of Agriculture (USDA) food pattern, and AHA diet for dietary recommendations [53]. The 2016 ESC/EAS guideline also emphasizes the importance of healthy food choice [6].
In Korea, few studies have examined the association between dyslipidemia and dietary patterns, but diets rich in whole grains, such as brown rice and whole wheat, with vegetables, legumes, fish, fruits, and dairy products may be helpful. Many Korean adults consume a typical high-carbohydrate low-fat diet compared to Western populations. Therefore, increasing the proportion whole grains instead of refined rice and balanced diet including adequate amounts of fish, beans, and fresh vegetables would be beneficial. Furthermore, although fresh fruits and milk are recommended, fruit concentrates and sweetened milk should be avoided. Table 6 shows a list for food choice, and Table 7 shows an example of the recommended daily meal plan. The dietary guideline to prevent and manage dyslipidemia for Koreans is summarized in Fig. 7.
Physical activity: recommendation
Exercise and dyslipidemia
Whether exercise influences blood lipid level is controversial. This is because various results have been reported depending not only on the subjects’ sex, age, race, and lipid concentration but also on the type, amount, intensity, duration, and frequency of exercise, as well as on whether lifestyle and body weight changed with regular exercise [58]. Furthermore, exercise itself has little effect on lipid concentrations.
There are different types of exercise, including aerobic, resistance, and flexibility exercises. Aerobic exercise is a type of exercise that increases the body’s oxygen consumption during exercise and improves cardiopulmonary endurance. Some examples include speed walking, jogging, swimming, and cycling. Resistance exercise refers to exercise in which muscle strength is used to work against a weight or force, and this type of exercise increases muscle strength and muscle mass. Flexibility exercise increases the range of motion of major muscles and improves postural stability and balance through muscle stretching.
In general, aerobic exercise decreases triglyceride concentration while increasing HDL-C, with little changes to LDL-C concentration [59,60]. There is no debate in that exercise therapy prevents CVD, and CVD prevention is the major goal of dyslipidemia management. Therefore, exercise therapy is important for patients with dyslipidemia [58,61]. Exercise has been reported to lower the risk of CVD as well as CVD mortality and all-cause mortality by not only improving lipid metabolism but also stabilizing blood pressure, improving insulin sensitivity, improving inflammation indices, lowering body fat, strengthening cardiopulmonary capacity, improving cardiac muscle function, promoting ischemic pre-conditioning of cardiac muscles, improving vascular endothelial functions, improving myocardial flow, and having anti-thrombotic effects [62,63].
The effects of resistance exercise on lipids have been debated [64,65]. However, resistance exercise could be useful because increasing muscle mass and muscle strength can increase physical activities and improve activities of daily living in the elderly [58].
Exercise prescription
There is no particular exercise prescription for controlling dyslipidemia and the prescriptions are similar to those for CVD prevention [58,63,66]. In general, at least 150 minutes of moderate intensity aerobic exercise per week is recommended [63]. Exercise should be performed 4 to 6 days a week and at moderate intensity, which is about 55% to 75% of the maximum heart rate (= 220 − age) is appropriate. However, CVD patients taking β-blockers or non-dihydropyridine calcium channel blockers that markedly lower heart rate must not use the target heart rate. For these patients, the intensity should be set through an exercise stress test, but if no exercise stress test was performed, exercise should be started at a “moderate” level and maintained at “somewhat hard” level. Exercise should consist of 5 to 10 minutes of stretching and light walking as warm-up and 30 to 60 minutes of main aerobic exercise. Each session could be divided into shorter durations depending on one’s abilities. After exercise, a cool down with 5 to 10 minutes of light walking and stretching is needed (Table 8).
Resistance exercise should be performed twice a week, but intensity should be set according to age and conditions. In general, it is recommended to perform 8 to 10 exercise involving major muscle groups for at least 1 set of 8 to 12 repetitions each [61,63].
Smoking cessation: recommendation
| Content | Strength of recommendation | Level of evidence |
|---|---|---|
| Smoking cessation is strongly recommended, as smoking increases the risk for dyslipidemia and CVD. | I | A |
Smoking increases plasma free fatty acid levels through enhanced lipolysis, which results in insulin resistance. Furthermore, smoking impairs reverse cholesterol transport [67-69]. According to a meta-analysis, total cholesterol, triglyceride, VLDL-C, and LDL-C concentrations are 3%, 9.1%, 10.4%, and 1.7% higher, respectively, and HDL-C concentration is 5.7% lower among smokers than among non-smokers [70]. After quitting smoking, blood HDL-C is significantly increased [71,72].
Smoking is a strong risk factor for CVD. The risk associated with smoking is related to the amount of smoking with no lower limit for deleterious effects [73]. Reducing the amount of smoking is not recommended, as it does not increase the possibility of smoking cessation and actually makes it more difficult to quit smoking [74]. Furthermore, passive smoking also increases the risk of CVD [75]. A meta-analysis and RCT confirmed that smoking cessation lowers the incidence and mortality of CVD [76,77].
Therefore, smoking cessation is strongly recommended to prevent dyslipidemia and CVD.
PHARMACOLOGICAL THERAPY FOR DYSLIPIDEMIA
Guideline summary of pharmacological therapy for dyslipidemia
Selection of drugs
Pharmacological therapy in addition to therapeutic lifestyle modification, such as diet therapy, exercise, and smoking cessation, is important for the management of dyslipidemia. To determine whether to start drug therapy, a comprehensive consideration should be given to both the CVD risk and LDL-C level for each patient. The CVD risk is classified as low risk, moderate risk, high risk, and very high risk. Pharmacological therapy can be initiated according to established history of CAD, peripheral artery disease, and ischemic stroke and patients with atherosclerotic artery disease (aortic aneurysm, transient ischemic attack, carotid artery disease with significant stenosis) or diabetes as well as to the number of CAD risk factors (smoking, hypertension, low HDL cholesterolemia, family history of premature CAD, age). Statin is the first line drug for hypercholesterolemia and the dosage is recommended to be adjusted to reach the target LDL-C level. The primary treatment goal is to lower the LDL-C to the target level or below and the secondary goal is to lower non-HDL-C concentration to target or below. Prior to drug therapy, it is important to investigate and correct secondary causes that may increase LDL-C or triglyceride levels (Table 9). Table 10 describes selection of drugs according to dyslipidemia treatment standard.
Hypercholesterolemia
The major independent risk factor associated with improved prognosis in patients with dyslipidemia and CVD is the reduction of LDL-C. Statin has been proved to lower CVD morbidity and mortality in both primary and secondary prevention studies, and according to a meta-analysis, CVD mortality, cardiovascular events, and stroke decreases by 20%, 23%, and 17%, respectively, with every 39 mg/dL reduction of LDL-C [27]. Statin is the primary pharmacological agent for hypercholesterolemia, and the dose should be adjusted based on the patient’s CVD risk to meet the targeted LDL-C level (I, A) [24,78,79].
Very high-risk group are the patients with atherosclerotic CVD (CAD, peripheral artery disease, ischemic stroke, transient ischemic attack) are classified as the very high-risk group. For this group, the goal of treatment is to reduce LDL-C concentration to < 70 mg/dL or by more than 50% of the baseline for secondary prevention. Statin should be immediately administered regardless of baseline LDL-C concentration for patients with acute MI as well as patients who underwent revascularization therapy due to atherosclerotic ischemic heart disease. For the very high-risk group, use of PCSK9 inhibitors was proven to have cardiovascular protective effects, so PCSK9 inhibitors may be additionally used if the target LDL-C concentration is not achieved even after using maximum tolerable dose of statin and ezetimibe (IIb, A) [30,80].
High-risk group includes the patients with significant carotid artery disease, abdominal aneurysm, and diabetes. Statin treatment should be started if LDL-C is ≥ 100 mg/dL, and could be selectively considered even for patients with an LDL-C level of < 100 mg/dL. For patients with diabetes with target organ damage or major cardiovascular risk factors, the degree of risk could be elevated depending on the patient.
Moderate-risk group includes the patients with two or more CV risk factors. For these patients, statin therapy should be started when LDL-C is ≥ 130 mg/dL but could be started even for those with LDL-C level 100 to 129 mg/dL when patients have multiple CV risk factors.
Low-risk group includes the patients with one or fewer risk factors, stain therapy may be used if the patient’s LDL-C is ≥ 160 mg/dL. Drug therapy is used for the lowrisk or moderate-risk group if LDL-C concentration level persists to be above the treatment cut-off despite weeks or months of therapeutic lifestyle modification (IIa, B). Pharmacological treatment strategy for hypercholesterolemia is as follows (Fig. 8).
Hypertriglyceridemia
When triglyceride concentration is high, it is recommended to first determine whether there are other factors increasing triglycerides and then to establish the treatment plan by evaluating the cardiovascular risks (Table 9). For individuals with a triglyceride concentration of 500 mg/dL or higher, immediate drug therapy (I, A) and lifestyle modification are important to prevent acute pancreatitis. Life style modification in these patients need to change to a low-fat diet (reduce fat intake to 10% to 15% of total energy intake) and complete abstinence from alcohol. In addition, pharmacological therapy should be started, particularly using fibrate (I, B) or omega-3 fatty acids (IIa, B), which lower triglyceride levels [81-83]. For patients with diabetes, strictly regulating blood glucose level using insulin is helpful.
When the triglyceride level is between 200 to 499 mg/dL, the primary treatment goal is to lower the LDL-C to below the target on the basis of the calculated cardiovascular risk (I, A) and the secondary goal is to lower non-HDL-C to below the target (IIa, A). Therapeutic lifestyle modification and statin therapy should be considered (I, A). After achieving the target LDL-C goal through therapeutic lifestyle modification and statin therapy, when the triglyceride concentration is still > 200 mg/dL or non-HDL-C, triglyceride lowering drug therapy may be considered (IIa, B). Fibrate (I, B) or omega-3 fatty acids (IIa, B) should be used to control triglyceride levels [82,83] especially in high-risk and very high-risk groups. If the target triglyceride goal is not met with monotherapy, combination therapy may be considered (IIa, C) [84].
Low HDL cholesterolemia
Low HDL cholesterolemia is defined as HDL-C levels < 40 mg/dL. It is often observed in patients with type 2 diabetes, mixed dyslipidemia, chronic kidney disease, chronic liver disease, and autoimmune disease. Low HDL cholesterolemia is often found with hypertriglyceridemia. Low HDL cholesterolemia should be considered when assessing the overall CAD risk. In the Korean National Health and Nutritional Examination Survey from 1998 to 2010, hypertriglyceridemia and low HDL cholesterolemia are more common than hypercholesterolemia [85]. The primary treatment goal for low HDL cholesterolemia is to lower the LDL-C to the target level based on the patient’s CV (I, A). To increase HDL-C while lowering the LDL-C to the target, therapeutic lifestyle modification, such as smoking cessation, weight loss, and exercise, should be concurrently performed. In patients with low HDL cholesterolemia in the very high-risk or high-risk group, the use of agents that elevate HDL-C, such as fibrate or nicotinic acid, may be considered after controlling LDL-C, but the additional cardiovascular protective effects of these agents when combined with statin have not been confirmed in prospective randomized primary and secondary prevention studies. In particular, nicotinic acid products are not currently available in South Korea and treatment to elevate HDL-C is no longer recommended (III, A).
Characteristics of lipid-lowering drug
Statin: 3-hydroxy-3-methyl-glutaryl coenzyme A reductase inhibitor
Statin is currently recommended as the first-line pharmacologic agent among other therapeutic agents, as it has relatively few adverse effects and clearly is beneficial for reducing CVD by lowering LDL-C [86].
Mechanism of action
All statins decrease cholesterol synthesis by competitively inhibiting the cholesterol precursor, 3-hydroxy-3-methyl-glutaryl coenzyme A (HMG-CoA) reductase [87]. To maintain cellular cholesterol homeostasis, LDL receptors are elevated while cholesteryl ester formation is decreased. As a result, blood LDL-C is further removed and VLDL production in the liver is diminished, consequently lowering LDL. Statins not only block cholesterol synthesis but also inhibit the synthesis of lipid intermediates, which have important biological effects. Lipid intermediates, such as geranylgeranyl pyrophosphate and farnesyl pyrophosphate prenylate proteins, enable them to be attached to the cellular membrane and promote the biological activity of these molecules. One of the mechanisms through which statin increase HDL-C is by inhibiting the phosphorylation of peroxisome proliferator-activated receptor α, which regulates geranylgeranylation of Rho A and apo A1 transcription. Altering the prenylation of a protein appears to partially mediate the statin effects other than their LDL-C-lowering effect.
Types of statin
Seven types of stains, namely lovastatin, pravastatin, simvastatin, fluvastatin, atorvastatin, rosuvastatin, and pitavastatin, are currently used (Table 11).
Lipid-lowering effects
Statins vary in absorption, blood protein binding, elimination, and solubility and the LDL-C lowering effects also vary according to dose (Table 11) [85,88-91]. In general, increasing statin dose twofold decreases blood LDL-C by 6%. Furthermore, statin inhibits VLDL-C secretion in the liver, thus it lowers triglyceride levels by 22% to 45% in patients with hypertriglyceridemia. HDL-C is slightly (5% to 10%) elevated. Multiple studies on Koreans have reported the effects of each type of statin on lipid indices and some studies have shown that the same dose of statin leads to a greater reduction of LDL-C among Koreans than among foreigners (Figs. 9 and 10) [92-113].
Cardiovascular disease prevention research and indications
1) Secondary prevention of CVD
Patients with a history of CVD (angina, unstable angina, MI, stroke, transient ischemic attack) are known to be more vulnerable to relapse of cardiovascular event or mortality [102-104]. For these patients, it is recommended to use statins because these drugs prevent the recurrence of cardiovascular events (I, A) [24,36,114]. These patients are classified as a very high-risk group, and the goal is to reduce LDL-C to < 70 mg/dL or by > 50% of the baseline for secondary prevention. If MI occurs, immediately administer statin regardless of the baseline LDL-C concentration (I, A). Although there are not many large studies on Asians, preventive effects were greater in CVD patients younger than 75 years old for whom LDL-C was reduced by more than 30% to 50% using statin than in the group of patients whose LDL-C was reduced by a lesser degree using a different dose of statin. Therefore, it is recommended that moderate dose/moderate intensity or high dose/high intensity statin be used such that the baseline LDL-C concentration can be reduced by more than 30% to 50% (IIa, A) [24,27,115].
For CVD patients age > 75 years or older, statin therapy should be used after confirming potential interactions with the patient’s comorbidity or between drugs used (IIa, B) [24,116].
2) Primary preventive effects of CVD in the general population
Adults with a blood LDL-C concentration of 190 mg/dL or higher are likely to develop a CVD in their lifetime, so statin should be used if the blood LDL-C remains > 190 mg/dL even after appropriate lifestyle modification (I, A) [24,86,117,118].
For adults with blood LDL-C of 160 to 190 mg/dL, statin should be used if blood LDL-C remains > 160 mg/dL even after 4 to 8 weeks of appropriate lifestyle modification (IIa, B) [24,27].
For adults with blood LDL-C of 130 to 160 mg/dL, appropriate lifestyle modification should be made, and statin therapy should be determined to start in consideration of the risk for CVD (IIb, C) [24,27,119,120].
3) Primary preventive effects of CVD in patients with diabetes Patients with diabetes, carotid artery disease or aortic aneurysm are considered as high risk group. For these patients, statin treatment should be started for primary prevention when LDL-C is > 100 mg/dL (I, A) [24,117].
4) Effects of statin in patients with heart failure and patients undergoing hemodialysis
Statin does not have any preventive effects in patients with heart failure or in hemodialysis patients, so newly adding statin therapy is not recommended for patients beginning hemodialysis (III, B) [24].
Usage-dosage
Lovastatin: 20 to 80 mg/day, taken with dinner
Pravastatin: 10 to 40 mg/ day, evening administration is more effective
Simvastatin: 20 to 40 mg/ day, evening administration is more effective
Fluvastatin: 20 to 80 mg/day, evening administration is more effective
Atorvastatin: 10 to 80 mg/day, time of administration is not significantly relevant
Rosuvastatin: 5 to 20 mg/day, time of administration is not significantly relevant
Pitavastatin: 1 to 4 mg/day, time of administration is not significantly relevant
Adverse reactions
The most common adverse reactions are indigestion, heartburn, and abdominal pain, which occur in 4% and hepatotoxicity and muscle toxicity are rare but may be fatal [114]. For older adults aged ≥ 75 years, patients taking multiple drugs, particularly when taking drugs with the same metabolic pathway with statin, or in patients with comorbidities requiring multidrug therapy, such as heart transplantation/acquired immune deficiency syndrome, it is helpful to begin with a low dose and gradually increase the dose (IIa, C).
1) Hepatotoxicity: There is no need to stop drug administration when transaminase is slightly elevated. If transaminase is increased by more than three times the normal range, stop administration, and once normal levels are restored, restarting statin with a low dose or use another agent may be considered (IIb, C). If symptoms suggesting liver injury, such as fatigue, reduced appetite, abdominal pain, dark urine, and jaundice, manifest during statin therapy, liver function tests, including aspartate transaminase/alanine transaminase (AST/ALT), should be performed promptly (IIa, C) [24].
2) Muscle toxicity: The most common adverse reaction to statin is muscle pain [114]. About 10% of patients taking statin develop muscle pain and weakness and stop taking statin, but in many cases, it is uncertain whether the muscle symptoms are indeed caused by statin [121]. The incidence of muscle injury is reported to be 0.01% higher in the statin group than that in the control group. It is reported that muscle injury, defined as elevated muscle enzymes, rhabdomyolysis, hemoglobinuria, and acute kidney failure, occur in a small minority of patients. The risk for statin-induced muscle damage increases with multiple comorbidities or when statin is combined with cyclosporine, fibrate, macrolide antibiotics, and some antifungal agents [122]. Gemfibrozil especially increases the risk of muscle damage when combined with statin, but fenofibrate is known to have low risk. Regular measurement of muscle enzyme levels is not recommended for asymptomatic patients, as it has shown no benefits (III, A) [24]. However, for patients with muscle pain, stiffness, muscle knots, weakness, and general fatigue, it is recommended to check for muscle injury by measuring muscle enzyme levels (IIa, C) [24].
3) Diabetes: A recent study reported that statin increases new onset diabetes [120]. Most new-onset diabetes occurred in individuals who had glucose intolerance prior to taking statin and there is a possibility that it may occur more frequently in patients who had taken a high-dose of statin. Thus, checking fasting blood glucose is helpful prior to beginning statin therapy (I, B) [24]. Even for patients who developed diabetes after beginning statin therapy, it is better to continue taking statin and make necessary lifestyle modification, such as exercise, weight reduction, and smoking cessation, than to stop statin therapy altogether in order to prevent CVD (I, B) [24].
4) Cognitive impairment: There has been some report that cognitive impairment was observed among patients taking statin. Nonetheless, to date, it is more beneficial to check for adverse reactions of combined neuropsychiatric medications than to conclude that cognitive impairment is an outcome of statin administration (IIb, C) [24].
Contraindications
Active or chronic liver disease is an absolute contraindication. Statin administration should be stopped immediately once pregnancy is confirmed or in lactating woman. Combination with cyclosporin, macrolide antibiotics, antifungal agents, and cytochrome P-450 inhibitors is a relative contraindication and must be determined with caution.
Follow-up observation before and after statin therapy
1) Pre-test: Prior to statin therapy, blood transaminase concentration (AST/ALT) should be measured (I, B) [24]. If ALT concentration is 3 times higher than the normal range prior to therapy, statin therapy should be initiated only after assessing and treating liver disease and confirming that liver functions have been improved [24]. Muscle enzyme CK should be measured as well, and if the concentration is three times higher than the normal range, identify the cause first and decide on whether to begin statin therapy [24].
2) Follow-up test after statin therapy: Assess cholesterol, triglyceride, and HDL levels about 4 to 12 weeks after statin therapy (I, B). If LDL-C is < 40 mg/dL in two consecutive measurements, consider lowering the dose of statin. Evaluation of liver function should be considered at 4 to 12 weeks after administration and every 3 to 12 months thereafter check statin effects and hepatotoxicity. Furthermore, the physician may prescribe a follow-up-test to ensure patient safety even in the absence of symptoms [24].
3) Effects of cessation statin therapy: Blood LDL-C level rises again about 2 to 3 months later and reverts back to the pre-treatment levels [116]. In addition, the CV protective effects of statin disappear from 1 to 2 days after stopping administration, so it is crucial to continue taking the drug. Particularly, multiple studies have reported that pausing statin therapy in the acute phase for patients with CVD, such as acute coronary artery syndrome or cerebral infarction, leads to poor outcomes.
Summary
Ezetimibe
Indications and action mechanism
Ezetimibe is commonly combined with statin therapy, as it lowers LDL-C by inhibiting cholesterol reabsorption in the small intestine (IIa, B).
Usage-dosage
Take 10 mg of ezetimibe once a day. There is no relevant time of administration.
Follow-up test
Blood lipid profile may be tested every 3 to 6 months.
Adverse reactions
The most common adverse reactions to ezetimibe monotherapy are abdominal pain, diarrhea, flatulence, and fatigue and other uncommon adverse reactions include indigestion, gastroesophageal reflux, reduced appetite, arthralgia, muscle spasm, and chest pain. In blood tests, elevation of transaminase, gamma-glutamyl transferase (GT), and CK have been reported.
Contraindications
Ezetimibe is prohibited for individuals who show hypersensitivity to this agent. It is also prohibited for pregnant and lactating women, as its safety has not been established. It is also prohibited for patients with acute liver disease or moderate to severe chronic liver dysfunction.
Summary
Fibrate
Indications
Fibrate are used as monotherapy (I,B) or combination therapy with statin for hypertriglyceridemia (IIa,A).
Usage-dosage
Bezafibrate: 400 to 600 mg/day, 1 to 3 times a day, after meals
Fenofibrate: 160 to 200 mg/day, once a day, immediately after meals
Gemfibrozil: 600 to 1,200 mg/day, twice a day, 30 minutes before meals
Follow-up tests before and after treatment
Lipid profile, liver function test, kidney function test, general blood test, muscle enzymes (when there is unexplainable muscle pain or weakness)
Adverse reaction
The most common adverse reaction is indigestion, and cholesterol gallstones may occur more frequently. Myopathy may occur, but the incidence is not high. The risk for adverse reactions is elevated when kidney functions (estimated glomerular filtration rate [eGFR]) are reduced, as blood drug concentration is increased. In particular, combination therapy with gemfibrozil and statin increases the risk for myopathy. Fenofibrate is the preferred agent for combination therapy with statin, as it does not relatively increase the risk for myopathy. It binds to albumin, which increases warfarin concentration and, therefore, bleeding tendency, and it may also increase the effects of hypoglycemic agents [123].
Contraindications
Severe liver disease, gallbladder disease, and hypersensitivity to fibrate are absolute contraindications, and use of the drug requires precaution for individuals with reduced kidney functions [123].
Summary
Monoclonal antibody type PCSK9 inhibitors
Indications
For patients with familial hypercholesterolemia and the very high-risk group whose LDL-C levels do not reached to target LDL-C level despite statin monotherapy with maximum tolerable dose or statin and ezetimibe combination therapy, PCSK9 inhibitors may be combined with statin with or without ezetimibe (IIb, A).
Usage-dosage
Alirocumab: 75 or 150 mg via disposable pen or syringe
At first, subcutaneous injection of 75 mg in 2-week intervals or 300 mg in 4-week intervals. If not reached to target LDL-C level, dosage could be increased to 150 mg in 2-week intervals.
Evolocumab: 140 mg/mL via disposable syringe or automatic injector, or 420 mg/3.5 mL via disposable onbody infuser with a prefilled cartridge is injected subcutaneous in the abdomen, thigh, or upper arm (140 mg in 2-week interval or 420 mg in 1-month interval).
Inject 420 mg over 9 minutes using a disposable infuser or inject 140 mg three times consecutively within 30 minutes.
Follow-up test
Lipid profile, and liver function test every 3 to 6 months.
Adverse reactions
There may be adverse reactions in the injection site after subcutaneous injection of monoclonal antibody, but the reactions are generally mild, and other reactions include nasopharyngitis. PCSK 9 inhibitors are not known to increase hepatotoxicity, and compared to ezetimibe, there are is no elevation in muscle pain or CK levels. There are no known interactions with other drugs and adverse reactions from prolonged administration.
Contraindications
Hypersensitivity to alirocumab or evolocumab is an absolute contraindication.
Summary
Omega-3 fatty acids
Indications
Omega-3 fatty acids may be used alone for hypertriglyceridemia (IIa, B) or combined with statin for mixed hyperlipidemia (IIa, C).
Usage-dosage
Dosage that showed lipid-reduction effects was 2 to 4 g a day. This dose should be taken at once or at two split times.
Follow-up test
Lipid profile and liver function tests every 3 to 6 months.
Adverse reaction
There have been some reports of the occurrence of hemorrhagic stroke, elevated blood glucose, and elevated immunosuppression [124-132]. There have also been reports of nausea, vomiting, burps, fish-smelling burps, or fishy taste in mouth, as well as elevated liver indices, headache or itching, and arthralgia.
Contraindications
There are no contraindications other than hypersensitivity to the drug. The U.S. Food and Drug Administration classifies this drug as class C; thus, for pregnant women, the drug should be used only when there are clear benefits (II, C). Omega-3 fatty acids extracted from fish with incomplete purification or excessive intake pose a risk for heavy metal exposure, so it is not recommended for pregnant women. It is also not known if this drug is secreted in breast milk.
Summary
Nicotinic acid (niacin)
To date, studies have not found significant improvements of clinical outcomes after nicotinic acid and statin combination therapy, and there were actually more adverse reactions [133] Furthermore, there is no approved product available in South Korea, and niacin and statin combination therapy is no longer recommended to increase HDL-C (III A).
Combination therapy
Adding another pharmacologic agent to statin can be considered if LDL-C remains high even after adequate statin administration and lifestyle modification or patient has mixed dyslipidemia.
Statin and ezetimibe combination therapy
Combination of statin and ezetimibe additionally lowers LDL-C by 15% to 20% compared to statin monotherapy. Ezetimibe (10 mg) and simvastatin (40 mg) combination therapy significantly reduced major cardiovascular events compared to simvastatin (40 mg) monotherapy in the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study that assessed simvastatin/ezetimibe therapy in patients with asymptomatic aortic stenosis, in the Study of Heart And Renal Protection (SHARP) on patients with chronic kidney disease, and in the IMPROVE-IT on patients with acute coronary syndrome [24,33,134-136]. As clinical trials proved, further lowering LDL-C by adding ezetimibe to statin therapy has benefits for improving clinical outcomes, so ezetimibe should be added if the target LDL-C goal is not met even with maximum tolerable dose of statin (IIa, B).
Statin and PCSK9 inhibitor combination therapy
PCSK9 inhibitors may be considered for very high-risk group if the target LDL-C is not met even with maximum tolerable dose of statin with or without ezetimibe or if the patient has statin intolerance. Two types of PCSK9 inhibitors, currently available evolocumab and alirocumab, lower LDL-C by 50% to 70% regardless of statin/ezetimibe therapy for hyperlipidemia [30,137,138]. Furthermore, FOURIER study proved that the evolocumab group had a 59% reduction of LDL-C with 15% less risk of combined primary outcome, including cardiovascular mortality, MI, cerebral infarction, hospitalization due to unstable angina, and coronary artery intervention [30]. Therefore, PCSK9 inhibitors may be combined with statin therapy for the very high-risk group if LDL-C remains high even after using maximum tolerable dose of statin (IIb, A).
Statin and fibrate combination therapy
In the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) and ACCORD studies that studied of statin and fenofibrate therapy in patients with diabetes, statin and fibrate combination therapy did not significantly lower cardiovascular risk, the primary endpoint of the study. However, in a retrospective subgroup analysis, the total CVD incidence was 27% lower in the dyslipidemia group, who had high triglyceride and low HDL-C [46,139,140]. Fibrate, when combined with statin, were found to be effective in lowering CVD risk in some high-risk patients with high triglyceride and low HDL-C levels; thus, additional studies are needed to prove the clinical efficacy. However, there may be an elevation of muscle-related symptoms and diseases as a result of fibrate and statin combination therapy, so clinicians should choose agents appropriately and be well aware of the indications.
Stain and bile acid sequestrant combination therapy
Combination of statin and bile acid sequestrants may be considered for achieving the target LDL-C goal. Adding bile acid sequestrants to statin therapy may additionally lower LDL-C by 10% to 20%. However, there has been no clinical trial assessing whether statin/bile acid sequestrant therapy decreases CVD, while a study using coronary artery angiography reported that it lowers atherosclerosis [141].
Statin and omega-3 fatty acid combination therapy
These two agents are generally used when aiming to lower both LDL-C and triglyceride levels (IIa, C). In some early studies, combining low-dose statin with eicosapentaenoic acid decreased major cardiovascular events compared to statin monotherapy, but multiple subsequent studies could not observe significant reduction of mortality with use of alpha-omega, supplementation with folate, vitamin B6 and B12 and/or omega-3 fatty acids, and other studies also did not find significant improvements of outcome [83,142].
Statin and niacin combination therapy
The “Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy,” the Atherothrombosis Intervention in Metabolic Syndrome with low HDL/HIGH Triglycerides (AIM-HIGH) trial reported [133] that statin and niacin combination therapy sufficiently controlled LDL-C in patients with CVD, but the study was prematurely terminated, as there were no significant improvements of outcomes in patients with atherogenic dyslipidemia after adding niacin (1.5 to 2 g/day) to statin therapy. However, this study also reported that it may lower CVD risk in patients with high triglyceride but low HDL-C levels. Unfortunately, niacin was associated with some adverse reactions such as elevated blood glucose, blushing, infection, and skin disease, and consequently, it became unavailable in some countries. Furthermore, the “Effects of extended-release niacin with laropiprant in high-risk patients,” HPS2-THRIVE study reported that adding niacin and facial flushing inhibitor laropiprant to statin therapy could not reduce major cardiovascular events and actually led to an increase of adverse reactions, such as myopathy, liver dysfunction, and increased risk of diabetes [143]. Therefore, statin and niacin combination therapy is not recommended (III, A).
DYSLIPIDEMIA IN SPECIAL GROUPS
Dyslipidemia in stroke patients
Dyslipidemia’s contribution to stroke varies across subtypes, and the association between dyslipidemia and ischemic stroke caused by atherosclerosis is the most well known. Dyslipidemia is an important risk factor for atherosclerotic ischemic stroke, and multiple clinical trials have shown that aggressive statin therapy can lower the incidence of stroke. Conversely, some cohort studies have also reported an association between low blood cholesterol levels and incidence and mortality of hemorrhagic stroke. Therefore, different approaches should be taken to treat dyslipidemia in stroke patients depending on the type of stroke involved.
Primary prevention of stroke and dyslipidemia
Elevated total blood cholesterol and LDL-C are risk factors for ischemic stroke and statin therapy is helpful for primary prevention of ischemic stroke [27,144]. In summary,
(1) Statin therapy is recommended for primary prevention of ischemic stroke for patients with a vascular disease or those at a high risk of CVD. The target LDL-C goal is set according to the general recommendations.
(2) For patients with a vascular disease, statin/ezetimibe combination therapy may be used for primary prevention of ischemic stroke.
Secondary prevention of stroke and dyslipidemia
Statin therapy for secondary prevention of stroke is the most effective for atherosclerotic ischemic stroke, and its preventive effects are yet unclear for other subtypes of stroke [32,145]. High-dose statin therapy has been associated with increased risk of bleeding in ischemic stroke patients with hemorrhagic stroke [32,146]. Considering the large number of hemorrhagic stroke patients in Korea, high-dose statin therapy should be used carefully. Although research data on the goal of dyslipidemia treatment for secondary prevention in stroke patients is yet thin, aggressive LDL-C correction is important for atherosclerotic ischemic stroke.
In summary,
(1) Dyslipidemia must be corrected for ischemic stroke patients and for secondary prevention of ischemic stroke, lifestyle adjustment, dietary therapy, and pharmacologic therapy, particularly statin therapy are recommended.
(2) High-dose statin therapy is recommended for secondary prevention of stroke for patients with ischemic stroke, atherosclerotic ischemic stroke, or transient ischemic attack with CVD. The treatment goal is to lower LDL-C to < 70 mg/dL or by more than 50% of the baseline level.
Dyslipidemia in patients with chronic kidney disease
Early phase of chronic kidney disease is characterized by elevated levels of triglyceride, reduced HDL-C, and increased LDL, particularly small dense LDL particles. As renal function declines, the rate of LDL-C breakdown is further slowed and, consequently, total cholesterol and LDL-C levels are elevated.
Unlike patients with normal kidney function, the primary or secondary prevention effects of statin on CVD are yet unclear for patients with chronic kidney disease. The 2013 The Kidney Disease: Improving Global Outcomes (KDIGO) guidelines recommended to remove LDL-C as a criterion for assessing appropriateness of treatment target in the management of dyslipidemia for patients with chronic kidney disease and instead proposed the use of future cardiovascular risk (rates per 1,000 person years) [147].
Usage and dosage
The same pharmacologic agent/dose used for healthy counterparts is permitted for patients with chronic kidney disease with an eGFR of ≥ 60 mL/min/1.73 m2 (excluding patients who had kidney transplantation). There are no clear data on the safety of high-dose statin in patients with chronic kidney disease with an eGFR of < 60 mL/min/1.73 m2, and there may be potential adverse reactions. Hence, the documented dose in largescale studies is recommended for these patients (Table 12) [135,148-150].
Approach to dyslipidemia in patients with chronic kidney disease
There is no direct evidence that performing blood lipid test at the time of diagnosis with chronic kidney disease is helpful for the patient’s outcomes. However, blood lipid testing is recommended, as it is relatively cheap and is helpful for detecting and distinguishing secondary dyslipidemia, such as that caused by hypothyroidism, excessive drinking, nephrotic syndrome, diabetes, liver disease, and use of other corticosteroid. Uniform and regular follow-up tests for LDL-C are not recommended after the diagnosis of chronic kidney disease. However, individual follow-up tests may be needed depending on the patient, such as for assessing patient adherence, considering change of dialysis method, diagnosing other secondary dyslipidemia, or assessing 10-year cardiovascular risk in patients under the age of 50 to begin statin therapy.
Cholesterol-lowering drug therapy in adult patients with chronic kidney disease
Regarding cholesterol-lowering therapy for patients with chronic kidney disease, the 2011 guidelines by ESC/EAS stresses that chronic kidney disease is considered a CAD risk equivalent and lowering LDL-C is the primary treatment goal for these patients [151]. The 2013 KDIGO guidelines suggest classifying individuals with a 10% or higher 10-year risk for coronary death or non-fatal MI as the statin therapy group [147]. Among patients with chronic kidney disease, those aged 50 years or older are recommended to undergo statin/ezetimibe or statin monotherapy regardless of their eGFR. For patients under the age of 50 years, statin or statin/ezetimibe is recommended if the patient has a history of CAD, diabetes, or ischemic stroke or if the 10-year risk for CAD mortality or non-fatal MI exceeds 10%.
For patients with chronic kidney disease requiring maintenance dialysis, newly adding statin therapy is not recommended, as statin was not found to have significant effects in three large-scale prospective randomized controlled studies [135,149,150]. Although it is not clear whether individuals on statin therapy prior to dialysis should stop statin therapy, it is necessary to analyze the risk/effects for continuing statin in consideration that statin is less effective on these patients compared to non-dialysis patients.
Among patients with chronic kidney disease who had a kidney transplantation, the incidence of CAD is very high compared to that of the normal population, at about 21.5 events/1,000 patient-year [148]. In the same study, fluvastatin reduced, though statistically insignificant, the incidence of CAD by 17% in those patients. For the treatment of lipid abnormality, statin is the recommended first-line treatment, but it should be started at a low dose and be increased gradually. Considering pharmacologic interactions, fluvastatin and pravastatin are recommended for transplant patients taking cyclosporine [6].
Triglyceride-lowering drug therapy for adult patients with chronic kidney disease
Therapeutic lifestyle modification should be considered first. Using fibric acid derivatives, which had been recommended in previous guidelines for the prevention of pancreatitis, is no longer recommended, as the supporting evidence is very weak. However, fibric acid derivatives may be considered for those with a fasting triglyceride of ≥ 1,000 mg/dL, and if used, the dose should be appropriately adjusted depending on the patient’s kidney functions. In such cases, patients are considered at a high risk for adverse reactions, so combination therapy with statin is not recommended. A large meta-analysis on the general population reported that fibrate therapy decreased major cardiovascular events and coronary events by 10% and 13%, respectively [45]. However, the effects are relatively weak compared to that of statin, and it elevates serum creatinine levels; thus, fibrate is not recommended for the purpose of lowering cardiovascular risks for those with chronic kidney disease [152]. In addition to pharmacological therapy, non-pharmacological therapy, such as dietary therapy, weight loss, increasing physical activity, lowering alcohol consumption, and blood glucose control, should be performed.
Adverse reactions and contraindications
Statin therapy in patients with stage 3 or higher chronic kidney disease may increase the risk of adverse reactions such as drug overdose and increased blood drug concentration, so choosing pharmacologic agents with low renal excretion is desirable (Table 11) [153]. Furthermore, using drugs that are not metabolized by CYP-3A4 enzymes would lower adverse reactions caused by drug interactions.
In general, fibric acids are not recommended for patients with chronic kidney disease, but they may be considered in special cases. In such cases, the dosage should be adjusted based on patient’s renal functions, and it should be noted that fibric acids may increase serum creatinine levels and that combining with statin may increase the risk of rhabdomyolysis [154,155].
Dyslipidemia in patients with diabetes
The risk of CVD is substantially increased with metabolic syndrome or diabetes, and CVD is one of the leading causes of death among patients with diabetes [156]. Because CVD mortality is about two to four times higher among patients with diabetes than among those without diabetes, dyslipidemia in these patients should be treated aggressively [157].
Typical diabetic dyslipidemia is characterized by hy pertriglyceridemia and decreased HDL-C. Furthermore, it is associated with an increased risk of atherosclerosis even without a high LDL-C, as small and dense LDL particles increase. Therefore, patients with diabetes are recommended to measure a lipid profile at the time of diagnosis and every year thereafter. In addition to the routine lipid tests (total cholesterol, HDL-C, LDL-C, triglyceride), non-HDL-C or apoB may be measured to assess diabetic dyslipidemia [158].
The present guidelines for the management of dyslipidemia classifies patients with CVD as the very highrisk group regardless of diabetes and recommends aggressive regulation of LDL-C to < 70 mg/dL for this group. For patients with diabetes without CVD, the goal of LDL-C < 100 mg/dL is recommended, but for those patients with CVD risk factors or target organ damage, such as proteinuria and chronic kidney disease, the target LDL-C may be further lowered to < 70 mg/dL.
Patients with diabetes and dyslipidemia need to engage in aggressive lifestyle modification [159]. Individualized education needs to be applied to each patient. For patients with diabetes who have poor glycemic control and high triglyceride levels, optimizing glycemic control is helpful for controlling dyslipidemia. Statin is the first-line treatment for patients with diabetes and dyslipidemia. In a study on patients with diabetes, statin therapy significantly contributed to both primary and secondary prevention of CVD [160,161]. If the target LDL-C goal is not met with the general statin dose, the dose should be increased to maximally tolerable dose or be substituted by high-intensity statins. Discontinuation of therapy was found to aggravate dyslipidemia in type 2 diabetes, so maintenance therapy is crucial, and confirming the continuity of medication is also essential [162].
Whether lowering triglyceride and increasing HDL-C with statin/fibric acid derivative therapy are beneficial for patients with type 2 diabetes is controversial. The ACCORD study found that statin/fibric acid derivative therapy did not significantly lower the incidence of CVD compared to statin monotherapy. However, in a subgroup analysis, the ACCORD study suggested that statin/fibric acid derivative therapy may have CVD preventive effects in patients with triglyceride ≥ 200 mg/dL and an HDL-C < 34 mg/dL [50,163].
In the IMPROVE-IT conducted on 18,144 patients who were admitted for acute coronary syndrome within 10 days of the study, simvastatin/ezetimibe therapy reduced relative risk for CVD by 6.4%. In the subgroup analysis, relative risk was reduced by 14% in the diabetes group, showing a greater CVD preventive effect among patients with diabetes [29]. Adding PCSK9 inhibitors, namely evolocumab or alirocumab, to patients with high CVD risk who are using maximum statin dose lowered LDL-C by 36% to 59% [164,165]. Based on these studies, adding ezetimibe or PCSK9 inhibitor may be considered for patients with diabetes and CVD if the target LDL-C goal is not met with maximum tolerable dose of statin.
Older adults and dyslipidemia
South Korea has already become an aged society in 2017, as the older adult population (≥ 65 years) reached 14% of the total population and it is expected to become a super-aged society by 2026, with the older adult population estimated to exceed 20% [166]. As a result of the growing elderly population, the prevalence and mortality of CVD are also expected to rise continuously. In particular, the prevalence of dyslipidemia increases among the elderly and many older adults are in the high-risk group for CVD; thus, lipid-lowering therapy is expected to be highly beneficial.
The primary preventive effects of statin on older adults aged ≥ 70 years have been proven to lower CVD and CVD mortality in a study of subjects aged 70 years or older and in a subgroup analysis of several large-scale studies [116,167,168]. Furthermore, the subgroup analyses on older adults in studies that attempted to examine the secondary prevention effects of statin therapy also found that statin significantly lowered the incidence of CVD without safety problems [169,170]. Therefore, statin therapy is recommended for primary and secondary prevention of CVD for older adults. However, evidence supporting the association between cholesterol levels, CVD, and mortality as well as the efficacy of statin therapy in patients excluded in these clinical trials, such as older adults aged ≥ 80 years or frail older adults, is lacking.
Because elderly patients often have multiple comorbidities and reduced organ functions, they are expected to have exhibited pharmacological differences in drug absorption, distribution, metabolism, and excretion, which may increase the risk of adverse drug interaction. However, current clinical trials of statin therapy did not find a significant increase of adverse reactions, such as rhabdomyolysis or increased liver enzyme levels, in older adults. Because many elderly patients have multiple comorbidities or take multiple medications, statin should be used while carefully monitoring its interactions with other drugs and its adverse reactions.
Dyslipidemia in children and adolescents
For Korean children and adolescents, dyslipidemia is defined as total cholesterol ≥ 200 mg/dL, LDL-C ≥ 130 mg/dL, non-HDL-C ≥ 145 mg/dL, triglyceride ≥ 130 mg/dL (chil dren below age 10, ≥ 100 mg/dL), and HDL-C < 40 mg/dL according to the 2011 National Heart, Lung, and Blood Institute (NHLBI) guideline (Table 13) [171]. However, according to the fourth National Health and Nutrition Examination Survey (2007 to 2010), triglyceride levels of 130 mg/dL falls under the 75th to 90th percentile and 150 mg/dL falls under the 90th percentile for Korean children and adolescents, which differs from the NHLBI’s definition of dyslipidemia. This may be attributable to the fact that a carbohydrate-based diet is the typical staple in South Korea, but additional studies are needed to substantiate the criteria for hypertriglyceridemia for Korean children and adolescents.
In general, a screening test is not recommended for children under the age of 9, and non-HDL-C that does not require fasting is recommended for children aged 9 to 11 years and adolescents aged 17 to 21 years. Children not in these age groups are recommended to undergo fasting lipid test if they present a risk factor for dyslipidemia or have family members with a risk factor (Table 14) [172-175].
Statin therapy should not be immediately initiated in children and adolescents even if dyslipidemia is discovered. The decision for drug therapy must be based on the mean results of two rounds of fasting lipid test performed in 2-week intervals within the past three months, and family history and risk factors must be assessed. In general, drug therapy is not performed in children under the age of 10, and only lifestyle adjustment and dietary therapy (Cardiovascular Health Integrated Lifestyle Diet 1 [CHILD1] → CHILD2-LDL) is performed for about six months. However, statin therapy may be considered if LDL-C persists to be > 190 mg/dL [171-176]. Furthermore, drug therapy may be considered for patients with severe primary hyperlipidemia or risk factors for medical complications [177].
Three to 6 months of dietary therapy is applied for children and adolescents between the ages of 10 to 21 years with mean LDL < 250 mg/dL or triglyceride < 500 mg/dL. Those with a BMI in the 85th percentile should be encouraged to reduce calories by increasing physical activities and altering lifestyle [178]. If the target lipid concentration is not met even with these modalities, drug therapy may be considered (Fig. 11). If the target LDL-C has been met but non-HDL-C is > 145 mg/dL in children above the age of 10, statin agents, fibrates, or niacin may be considered, and the patients must be referred to a specialist [171,179]. If fasting triglyceride is between 200 to 499 mg/dL and non-HDL-C is > 145 mg/dL even after lifestyle adjustment and dietary therapy (CHILD1 → CHILD2-triglyceride), the use of omega-3 fatty acids may be considered [171]. There have been only a few cases of pediatric use of omega-3 fatty acid, but no safety problems have been reported thus far. Those with triglyceride levels > 500 mg/dL must consult a specialist, as they have a risk for pancreatitis.
Familial hypercholesterolemia
Heterozygous familial hypercholesterolemia
Traditionally, the prevalence of heFH is known to be 1/500 [180]. Since patients with heFH are exposed to high levels of LDL-C over their life-time, they have an obviously high-risk of CVD. Accordingly, it is definitely important to appropriately diagnose patients as early as possible and prevent vascular complications.
Diagnosis
A patient is likely to have heFH when they present with premature CAD at age of < 50 years (male) or < 60 years (female) or has family history of FH. Diagnosis can be made based on clinical criteria or DNA mutation. Clinical criteria include Simon Broome criteria (Table 15), Dutch criteria, and Make Early Diagnosis to Prevent Premature Deaths (MEDPED) criteria [181,182]. Cascade screening is recommended for family members of a diagnosed proband of heFH.
Treatment
1) Principles of management of heFH include lifestyle modification, lipid-lowering agents, and screening for atherosclerotic CVD.
2) First target of lipid lowering therapy is to reduce LDL-C by 50% of baseline levels. Thereafter, it is desirable to lower LDL-C to < 100 mg/dL (when the patient has no CAD or other major risk factors) or to < 70 mg/dL (when the patient has CAD or other major risk factors). However, the target is not frequently achieved in real world practice and reduction of LDL-C as much as possible with maximal tolerable treatment is often a practical objective [183].
3) It is recommended to attempt to achieve the LDL-C goal by maximal tolerable dose of statins, the first line drug. If the target is not achieved, ezetimibe can be added. A considerable proportion of patients cannot reach the target and cholesterol binding resins or PCSK9 inhibitors can be added as third line agents [6,184]. When patients experience adverse events related to statins, second line or third line agents can be used instead.
4) For children of parents with heFH, DNA testing is recommended when a gene mutation in the father or mother is identified. Otherwise, it is better that they undergo LDL-C measurement. Statin therapy can be started at the age of 8–10 years and the target is 135 mg/dL at age >10 years [6].
Homozygous familial hypercholesterolemia
The prevalence of homozygous familial hypercholesterolemia (hoFH) is known to be 1/1,000,000 or higher. Because the exposure of vessels of hoFH patients to lipid is more severe than that of heFH patients, the incidence of CAD under the age of 20 years is not uncommon.
Diagnosis
One of the most well known international criteria for hoFH is that of EAS (2014). It includes DNA mutation, LDL-C levels, and family history.
Screening of complications
For examination of CAD or aortic disease, it is desirable to consult to cardiologist. Regular screening for complications is recommended.
Treatment
The aim of treatment in hoFH is to reduce LDL-C as early as possible and as much as possible. Treatment targets are 100, 135, and 70 mg/dL in adults, children, and patients with atherosclerotic CVD, respectively. Lifestyle modification, statins (with ezetimibe), and LDL apheresis (if available) are essentials of treatment. LDL apheresis is recommended at the age of 5 years or at least at age 8 years. New therapeutics such as lomitapide, mipomersen, or PCSK9 can be added.
Cholesterol during pregnancy
Changes in lipid metabolism during pregnancy
Lipids in plasma during pregnancy decrease at the first stage and then begin to increase after gestational age (GA) of 8 weeks. Increased insulin resistance and estrogen stimulation are responsible for the maternal hyperlipidemia observed during pregnancy [185]. In the first and second trimesters, fat accumulates due to increased food intake and lipogenesis; however, fat accumulation decreases during the third trimester because of enhanced lipolytic activity and decreased LPL activity [186]. In the later period of pregnancy, insulin resistance increases lipolysis, gluconeogenesis, and ketogenesis in the fasting state in pregnant women. Insulin increases the activity of LPL in adipose tissue and reduces the activity of hormone-sensitive lipase, which is a lipolytic enzyme. In addition, insulin inhibits hepatic gluconeogenesis and ketogenesis. Peripheral insulin resistance develops in women with gestational diabetes and plays a role in increasing blood nonessential fatty acids and ketone body concentration [187].
Hyperlipidemia during pregnancy
In the later period of pregnancy, triglycerides, phospholipids, and cholesterol levels increase. In particular, the increase of triglycerides is most prominent. Whereas HDL-C increases after the GA 12 weeks of pregnancy due to the increase of estrogen, the total cholesterol and LDL-C increase in the second and third trimesters. During pregnancy, hepatic lipase decreases the size of triglyceride-rich LDL-C and increases its density. Such changes damage endothelial cells and cause atheroma formation.
Treatment of dyslipidemia during pregnancy
Lifestyle modifications
Physical activity is effective in preventing gestational diabetes and gestational hypertension. The average triglyceride level, of any kind, is lower in women who are physically active. For diet therapy, it is difficult to make a definitive conclusion and additional studies are required.
Omega-3 fatty acid
Omega-3 fatty acids are elements of the diet and are not considered to increase adverse effects during pregnancy. There are insufficient data to recommend omega-3 fatty acid supplements instead of fish intake to normal pregnant women. However, supplementation of docosahexaenoic acid is recommended in pregnant women who do not usually eat fish at all.
Statins
Statins are contraindicated during pregnancy. Statins are not thought to increase fetal anomalies during pregnancy. Statin therapy is not recommended during pregnancy because there is no evidence that dyslipidemia treatment is beneficial to pregnant women or that cholesterol is required for the growth of embryo during pregnancy. A woman who is planning pregnancy or is already pregnant, should stop statins, if she is taking statins.
FUTURE RESEARCH TOPICS
Cardiovascular biomarkers
Carotid plaque and intima-media thickness
In addition to coronary artery calcification, carotid intima-media thickness is one of the most well-known surrogate markers of CVD [188]. Adding intima-media thickness to the traditional assessment of cardio-cerebrovascular disease using vascular risk factors enables a more detailed classification of risks [66,189].
Furthermore, carotid plaques are also considered an indicator of asymptomatic atherosclerosis [189]. Coronary plaque is associated with an elevated CVD risk, and a plaque of ≥ 4 mm in the aortic arch is a risk factor for stroke recurrence [188,190,191]. However, the increase in risk associated with coronary plaques is low [188,191].
According to a systematic literature review, statin therapy slows the increase of carotid intima-media thickness [192]. Furthermore, high-dose statin therapy is known to be more effective in treating carotid intima-media thickness and carotid plaques [193]. However, whether targeting the carotid intima-media thickness prevents CVD has not been confirmed. Similarly, studies examining whether carotid plaques can be the target of treatment are lacking. In the future, therapeutic efficacy should be investigated in more detail for high-risk groups (e.g., echolucent plaques or plaque ulcers).
Vascular calcification
Vascular calcification is commonly observed throughout the body among older adults. In the past, vascular calcification was believed to be a passive change that occurred with aging or harmless changes observed in atherosclerosis. However, recent studies have revealed that vascular calcification is associated with hypertension, dyslipidemia, diabetes, and renal diseases and that it is an actively regulated process similar to bone formation [194,195].
Calcification of various systemic arteries, including the coronary artery, carotid artery, aorta, and iliac artery, is associated, and may be mutually causally related with an elevation of systemic blood pressure, pulse pressure, and vascular stiffness [195-199]. Further, a systematic literature review reported that vascular calcification increases the risk for mortality, CAD, and cerebrovascular disease by two to four times [197]. Cerebrovascular calcification is most commonly observed in the intracranial internal carotid artery and it has been associated with cerebral small vessel diseases, which are a cause of dementia or stroke [200,201].
In particular, coronary arteries have been studied more extensively than other blood vessels. Coronary artery calcification generally occurs as a result of atherosclerosis and the amount of calcium deposited in coronary arteries is believed to be proportional to the total amount of atherosclerosis [202-204]. Furthermore, multiple studies have reported that coronary artery calcification is associated with vascular disease [203]. In a study that investigated the incidence of CVD in four racial groups, the risk for CAD was about 10 times higher in the group with a calcium score of 300 or higher compared to the group without coronary artery calcification [205]. In consideration of these findings, existing guidelines suggest the use of coronary artery calcification and its severity as an indicator for vascular disease risk and statin therapy [24,66,206].
However, despite mounting evidence, whether vascular calcification is an appropriate target of treatment is still doubtful. First, evidence supporting that vascular calcification is the sole cause of vascular diseases is lacking [188]. Second, although vascular calcification is related to the overall disease burden from atherosclerosis, coronary artery calcification is not directly proportional to the degree of stenosis of the coronary artery [204,207]. Coronary arteries without calcification may have stenosis and severely calcified coronary arteries may not have stenosis. Therefore, it is difficult to use coronary artery calcification as a surrogate index of vascular stenosis. Finally, effective treatment for vascular calcification has yet to be identified.
Subsequent studies should determine the causal relationship between vascular calcification and vascular diseases and develop treatment modalities for vascular calcification.
Novel serum markers of atherosclerosis
Atherosclerosis, a major cause of cardio-cerebrovascular disease, is a chronic inflammatory disease caused by injuries of vascular epithelial cells. Foreign treatment guidelines present inflammation and thrombus as novel serum markers of atherosclerosis [6,7,24]. However, the strength of recommendation is low due to a lack of adequate study findings and evidence for novel serum markers. Whether serum markers can be used for assessing the risk and treating cardio-cerebrovascular diseases requires further research.
In summary,
(1) There is insufficient evidence supporting the use of serum markers for atherosclerosis (e.g., hs-CRP, fibrinogen, lipoprotein-associated phospholipase A2 [Lp-PLA2], homocysteine) in the assessment of CVD risk in adults.
(2) Serum markers of atherosclerosis (e.g., hs-CRP, fibrinogen, Lp-PLA2, homocysteine) may be considered for assessing potential risk factors in order to determine the intensity of treating the risk factors for patients at moderate risk of CVD.
Development and validation of CVD risk assessment tool
The ACC/AHA cholesterol guideline uses CVD risk as an essential factor for determining drug therapy [24]. Table 16 compares the major CVD risk assessment tools developed in the United States and the risk factors and scope of diseases differ across the models. The ACC/AHA guideline adopted the Pooled Cohort Equations developed by the ACC/AHA Risk Assessment Work Group. This tool is characterized by the use of five community cohort data to increase the representativeness of the data and that the scope of target diseases was expanded to include acute MI, stroke, CAD mortality, and stroke mortality [208].
The 2016 ESC/EAS treatment guidelines mentioned the usefulness of CVD risk assessment. Although it recommends the use of the Systematic Coronary Risk Estimation (SCORE) system, it also introduced other risk assessment models, including Framingham, ASSIGN (CV risk estimation model from the Scottish Intercollegiate Guidelines Network), Q-Risk, Prospective Cardiovascular Munster Study (PROCAM), and the World Health Organization (WHO) [6]. The SCORE system was developed based on the data from 200,000 individuals in 12 cohorts across the European region, and separate charts were developed for low-risk countries and highrisk countries [209].
There have been studies in Korea aiming to develop risk assessment models to predict stroke, CAD, and overall CVD, and the Globorisk score also provides a risk assessment chart for Koreans [13,18,19,210]. However, treatment guidelines still do not recommend the use of these tools in the decision-making for drug therapy. There are concerns that the generalizability of these risk assessment tools developed in Korea needs to be further examined as they have not been adequately validated, while others are concerned that even if individual CVD risks are assessed, it is difficult to reflect them in treatment guidelines because evidence supporting the clinical efficacy and cost-effectiveness of drug therapy according to the level of risk is lacking. Additional studies on CVD risk assessment are needed to develop a guideline for the management of dyslipidemia appropriate for Koreans.
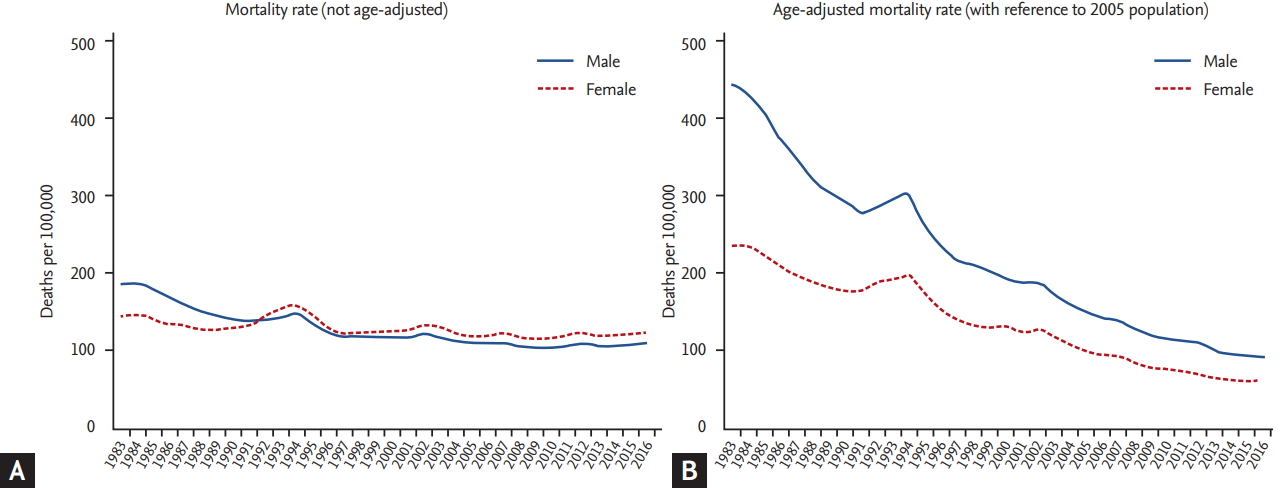
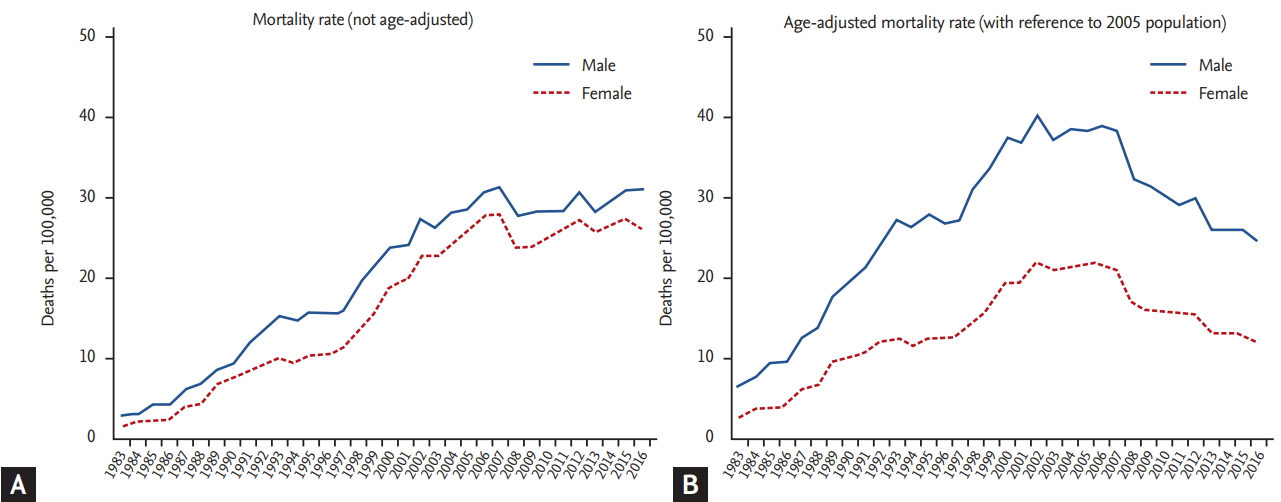
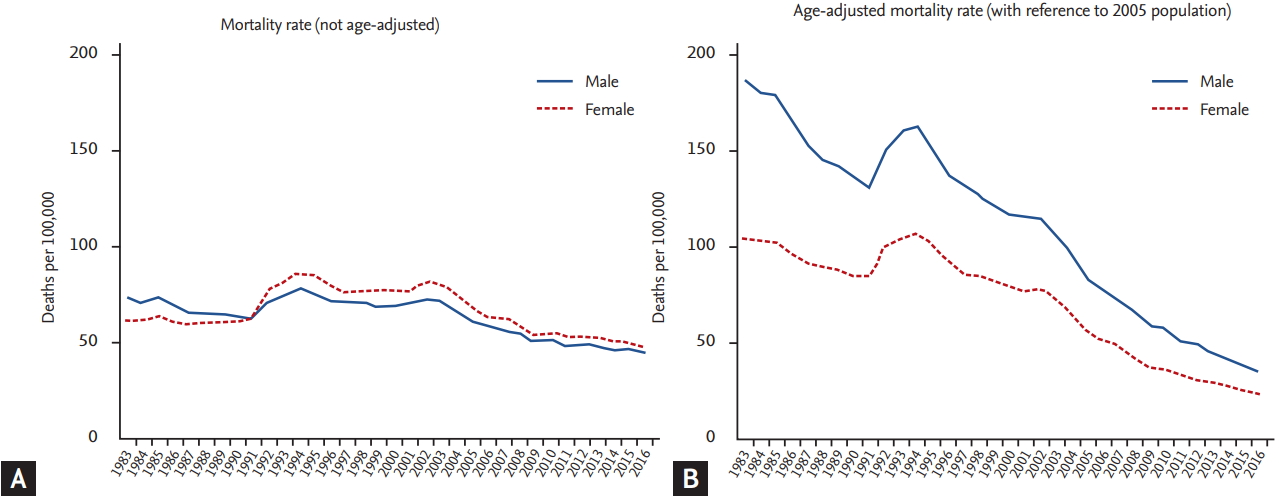
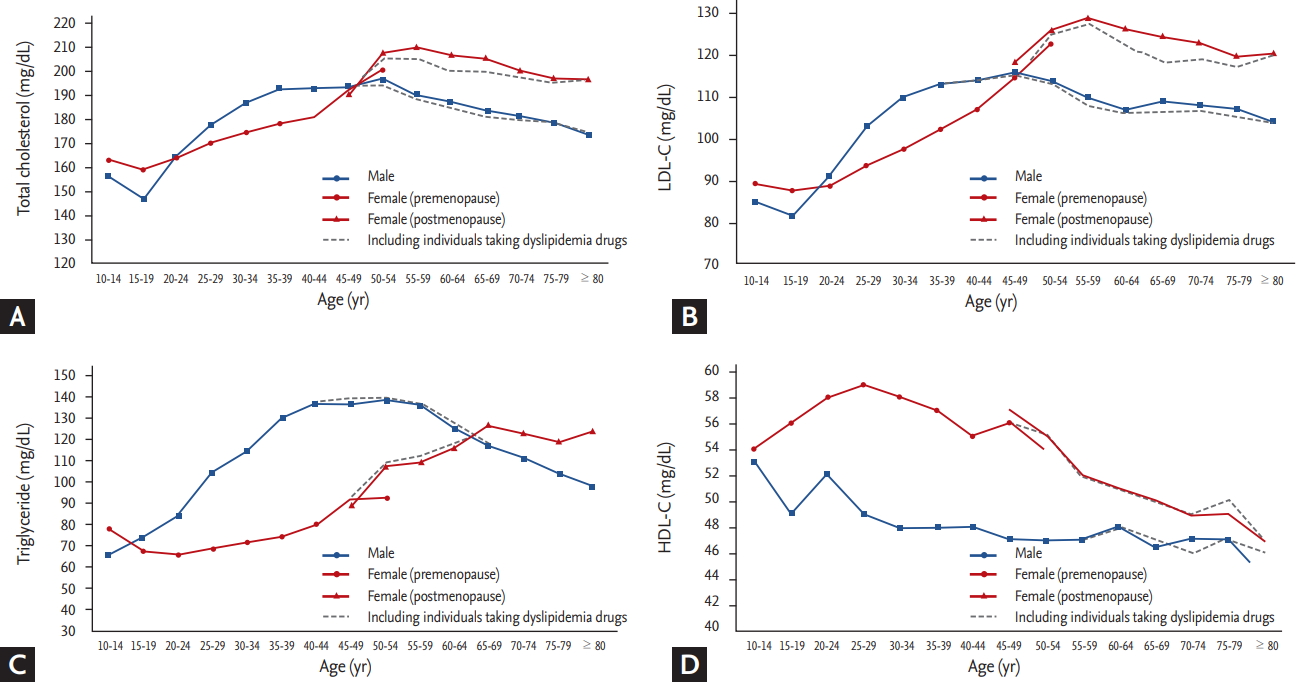
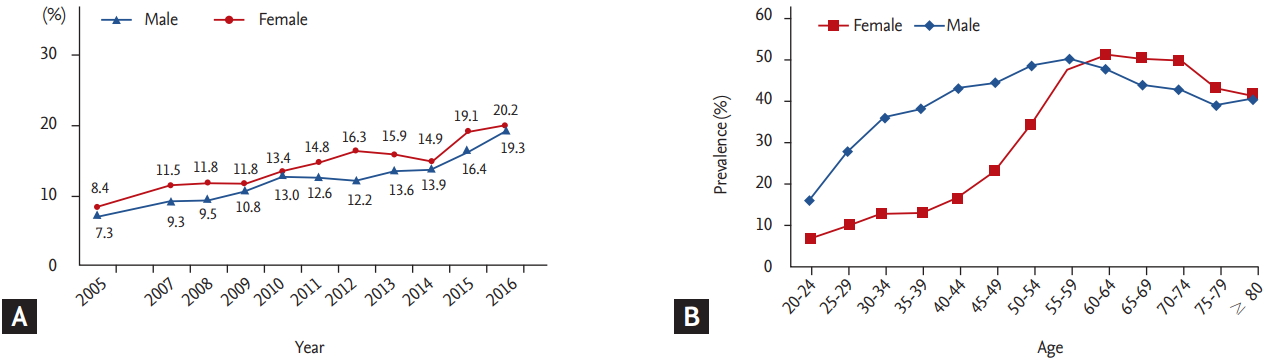
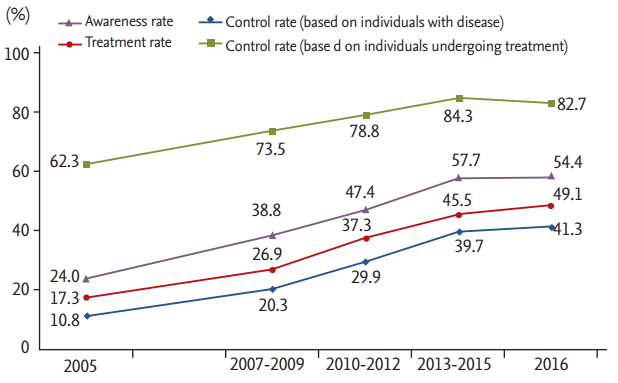
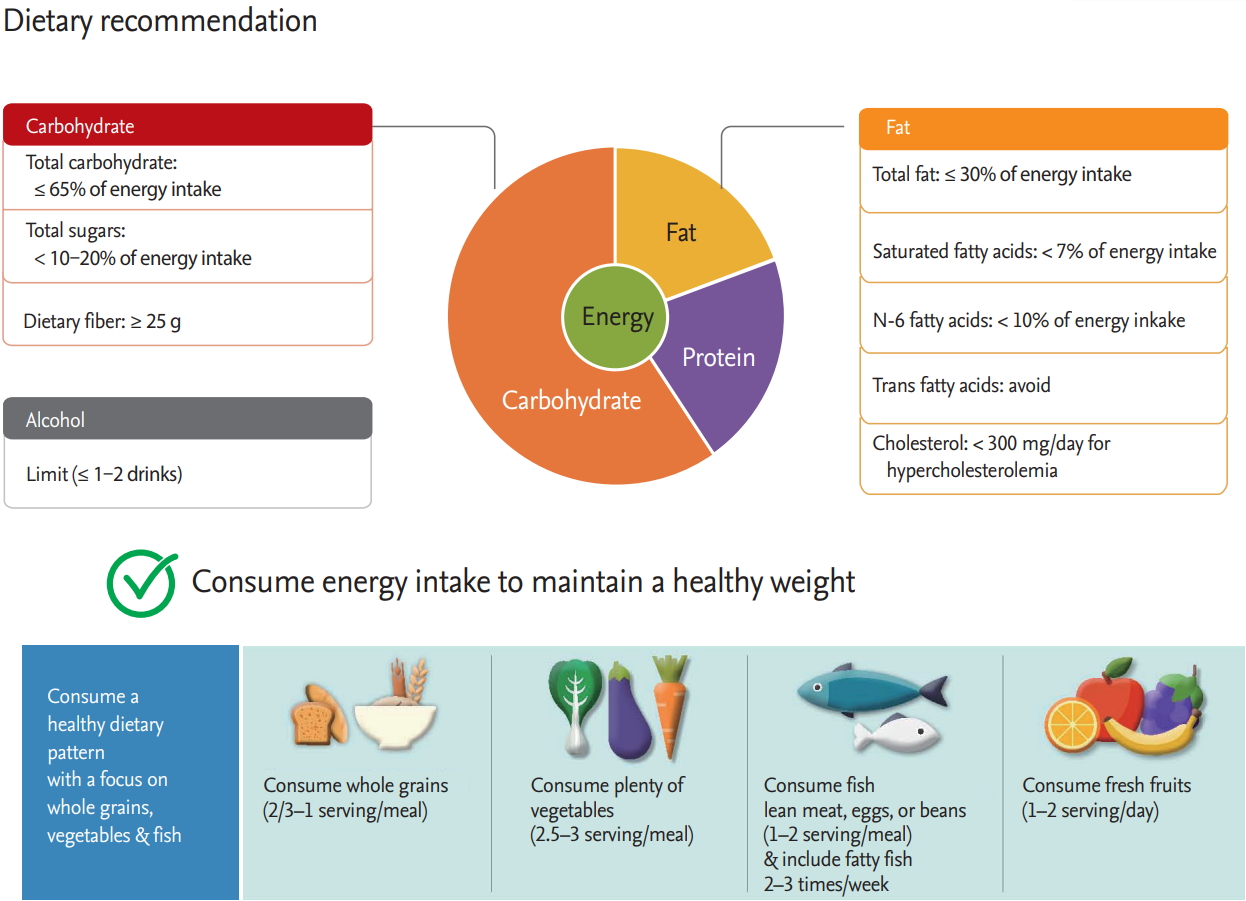
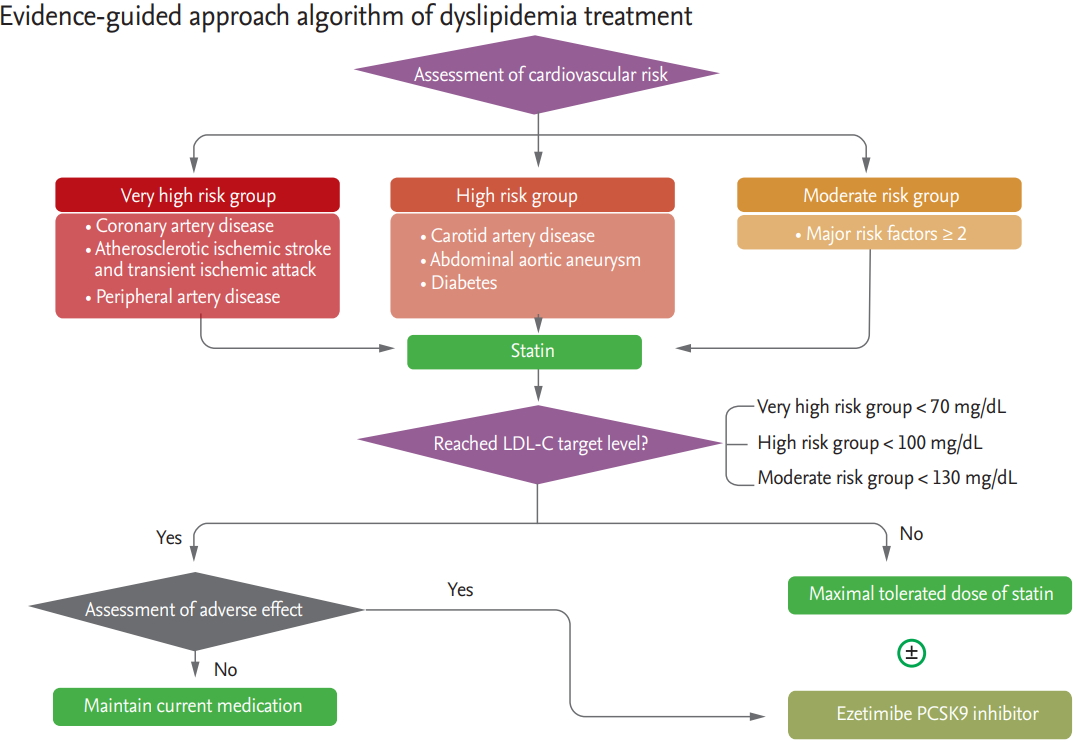

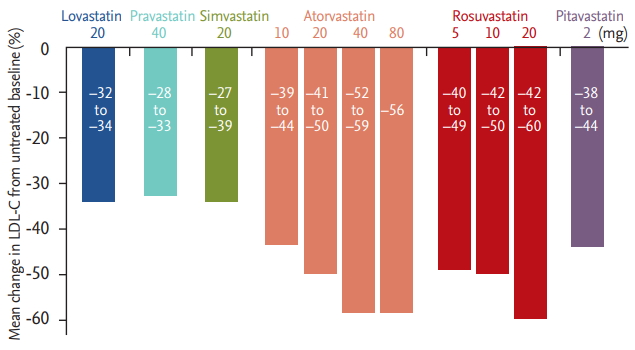
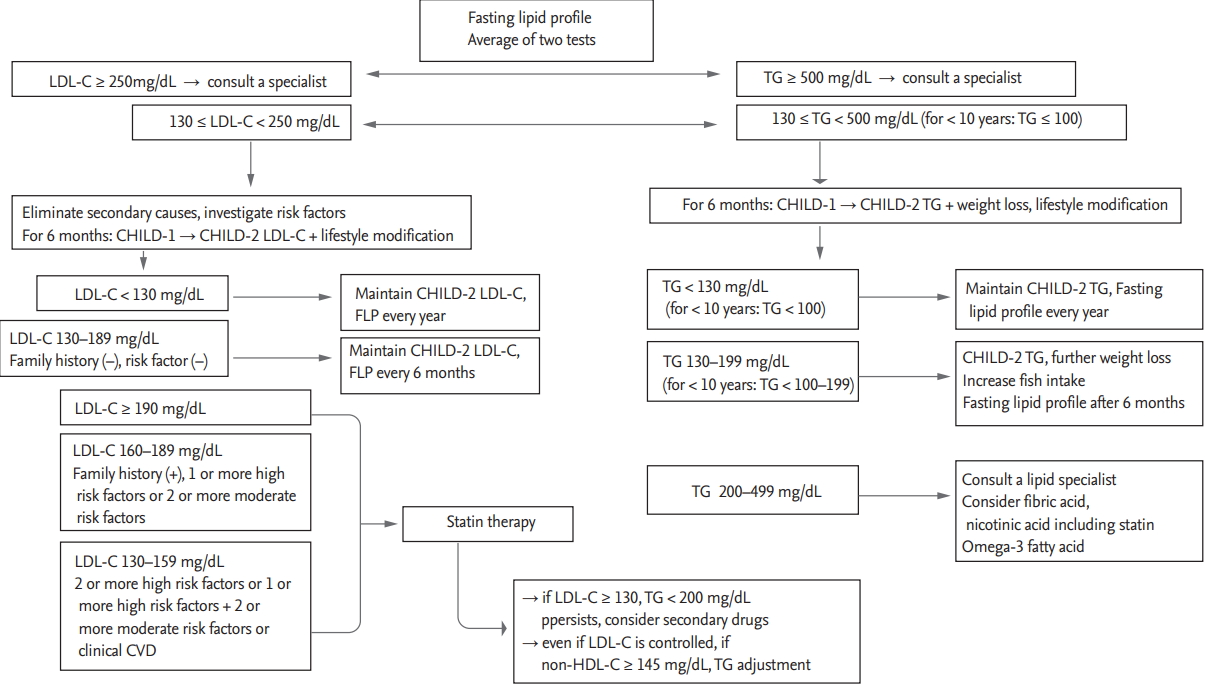
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





