


INTRODUCTION
Over the past few decades, treatment of chronic hepatitis B (CHB) patients has greatly improved with the development of effective oral nucleos(t)ide analogues (NAs), which inhibit reverse transcription of hepatitis B virus (HBV) polymerase [1,2,3]. The sustained suppression of serum HBV DNA to very low or undetectable levels by these drugs is associated with reduced hepatic inflammation, prevention of progression of liver fibrosis and inhibited progression to hepatocellular carcinoma (HCC) [4,5,6]. However, a major NA limitation is the development of drug resistance, which remains an obstacle to successful treatment of CHB patients, especially when they are treated sequentially with less potent and low genetic barrier drugs [7,8]. Reportedly, resistance to lamivudine (LAM), the first approved NA for treatment of CHB, occurs in up to 80% of patients after 5 years of treatment [9]. Switching to adefovir (ADV) monotherapy in LAM-resistant CHB patients led to the development of ADV resistant mutations in 18% to 25% of patients after 1 to 2 years of treatment [10,11,12]. Despite potent antiviral activity and a low rate of resistance development in treatment-naïve patients, entecavir (ETV) rescue therapy in LAM-resistant patients showed high rates of resistance [13,14,15]. As a result numerous patients have acquired resistance to multiple NAs, which has become a growing problem globally.
Tenofovir disoproxil fumarate (TDF) is an oral NA with the most potent activity against HBV and a high genetic barrier. TDF has been approved in the United States and Europe for the treatment of CHB since 2008. TDF has shown excellent treatment efficacy in treatment-naïve [16,17] as well as NA-experienced patients in various studies [18,19]. However, experience with TDF in Asian countries, especially in patients with multiple NA treatment failure, is quite limited. In Korea, a study of 29 patients who failed to respond to multiple NAs demonstrated 86.2 and 96.6% of a complete virological response (CVR) after 12 and 24 months, respectively, of tenofovir therapy at a median follow-up duration of 16 months [20]. However, due to the small number of patients and short follow-up duration, further studies are warranted to remedy the shortcomings of the pre-existing study in the Korean population. In this study, we evaluated the long-term efficacy and safety of TDF rescue therapy in a large cohort of Korean CHB patients after failure of multiple NA therapies.
METHODS
Subjects
In this study we enrolled CHB patients who received TDF therapy after treatment failure to at least two NAs between September 2008 and April 2013 at Samsung Medical Center (Seoul, Korea). NA treatment failure was defined as either a nonresponse (decreased serum HBV DNA < 2 log10 IU/mL after 6 months of therapy) or an incomplete response (persistent and measurable HBV DNA levels during NA treatment ≥ 6 months). Patients with serum HBV DNA levels ≥ 2.0 log10 IU/mL at the initiation of TDF treatment were enrolled. Exclusion criteria included coinfection with human immuno-deficiency virus or hepatitis C virus, a history of HCC and decompensated liver cirrhosis as defined by Child-Pugh scores > 7, the development of clinically evident complications of portal hypertension, including ascites, variceal hemorrhage, hepatorenal syndrome, or hepatic encephalopathy. The study protocol was approved by the Institutional Review Board of Samsung Medical Center, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Endpoints
The primary endpoint was defined as an HBV DNA level undetectable by real-time quantitative polymerase chain reaction (qPCR) during TDF treatment. Secondary endpoints were alanine transaminase (ALT) normalization, hepatitis B envelop antigen (HBeAg) seroclearance, safety and tolerability.
Definition of treatment response
CVR was defined as a decrease in serum HBV DNA to levels undetectable by qPCR. The primary nonresponse was defined as a decrease in serum HBV DNA of less than 2 log IU/mL after 6 months of therapy. Virological breakthrough (BT) was defined as an increase in HBV DNA of more than 1 log IU/mL compared with nadir. HBeAg seroclearance included HBeAg loss or seroconversion to anti-HBe.
Virological assay
Serum HBV DNA levels were measured by qPCR assay using the COBAS TaqMan HBV quantitative test (lower limit of detection at 9 IU/mL; Roche Diagnostic System Inc., Branchburg, NJ, USA). To identify mutations in HBV polymerase, PCR amplification and direct sequencing were performed as described previously [21]. In this study, LAM resistance was defined as the presence of rtL180M, rtM204V/I/S, or rtV173L. The presence of rtA181V/T, rtN236T, or rtN238A was defined as ADV resistance and the presence of rtT184A/I/L/S, rtI169T, rtS202G, or rtV207I as ETV resistance.
Clinical and laboratory assessments
Serum HBV DNA, HBeAg, ALT, creatinine and phosphorus levels were assessed routinely every 3 months during the TDF treatment. Information regarding drug adherence and laboratory data were collected retrospectively from medical records. Safety and tolerability were assessed from documented adverse events and laboratory abnormalities, such as azotemia, hypophosphatemia, hepatic decompensation, HCC development and death.
Statistical analyses
The cumulative probability of achieving undetectable HBV DNA was assessed using the Kaplan-Meier method. The difference between cumulative curves was tested using a log-rank test. Cox's regression model was used to analyze predictors of virological response. All p values were two-tailed, and a p < 0.05 was considered to indicate statistical significance. Statistical analysis was performed using SPSS version 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics of the study subjects
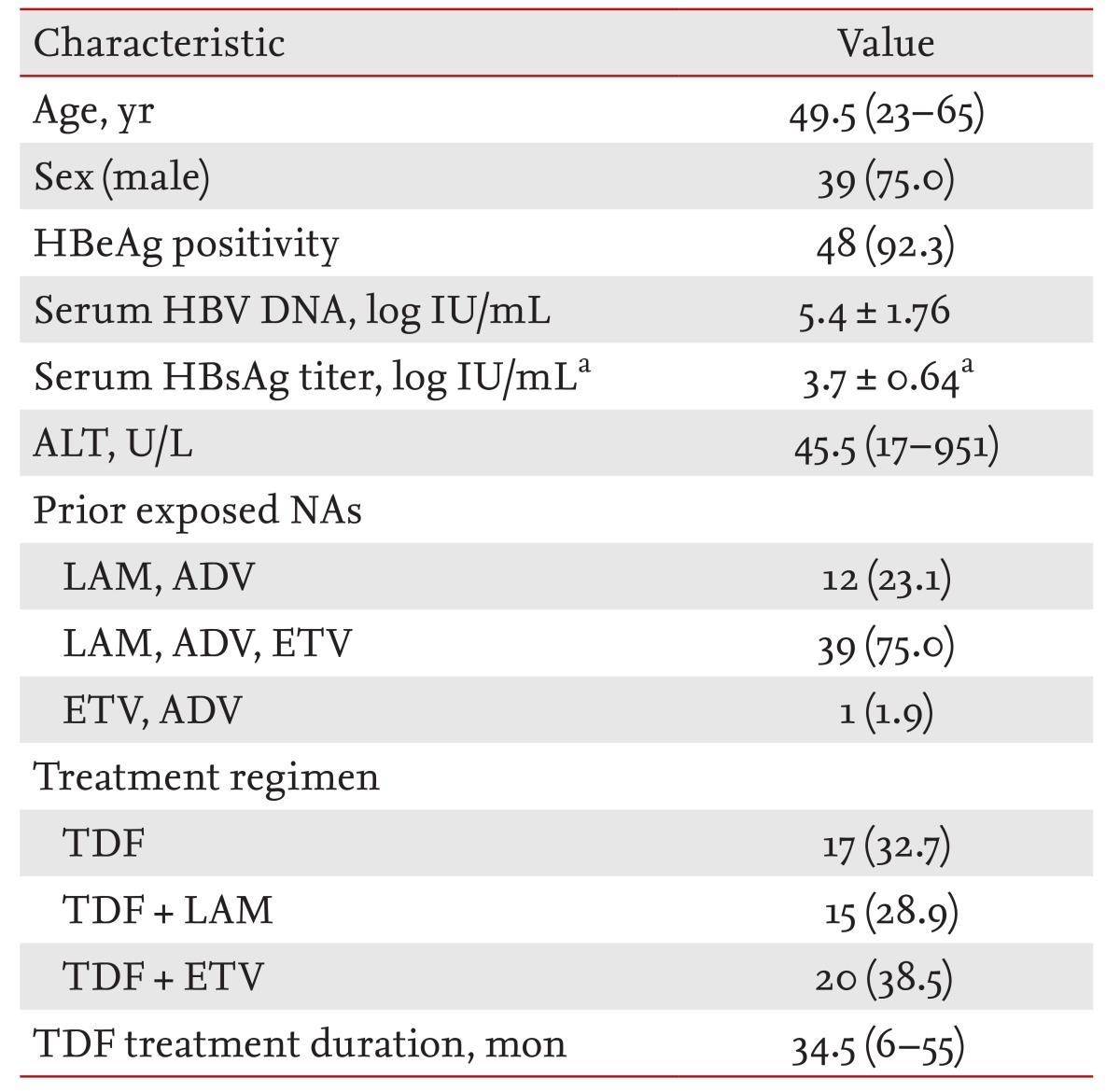
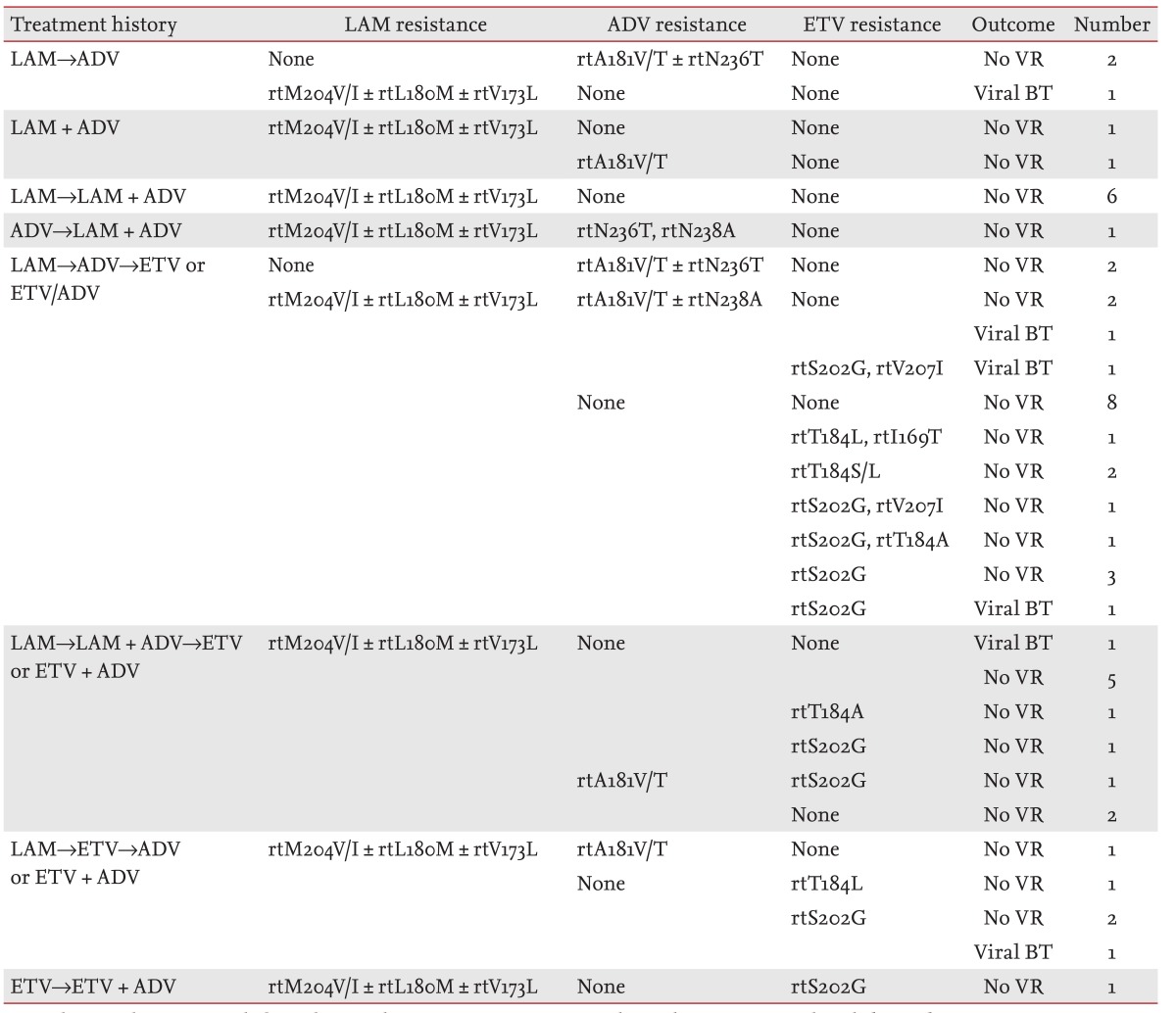
Baseline characteristics of the 52 patients are shown in Table 1. The median age was 49.5 years (range, 23 to 65), and 75.0% were male. The mean serum HBV DNA level was 5.4 ± 1.76 log IU/mL, and 48 patients were HBeAg-positive (92.3%). Serum samples from 50 patients were available for quantitative hepatitis B surface antigen (HBsAg) titers, and the mean serum HBsAg titer was 3.7 ± 0.64 log IU/mL. Seventeen patients (32.7%) were treated with TDF alone, 15 patients (28.9%) with TDF plus LAM and 20 patients (38.4%) with TDF plus ETV. Mutations associated with antiviral resistance against LAM, LAM/ADV, LAM/ETV, and LAM/ADV/ETV were identified in 22 (42.3%), 8 (15.4%), 16 (30.8%), and 2 (3.8%) patients, respectively. Detailed information regarding prior NA therapy history and genotypic resistance profiles is described in Table 2. The median duration of TDF treatment was 34.5 months (range, 6 to 55).
Antiviral efficacy of regimens containing TDF
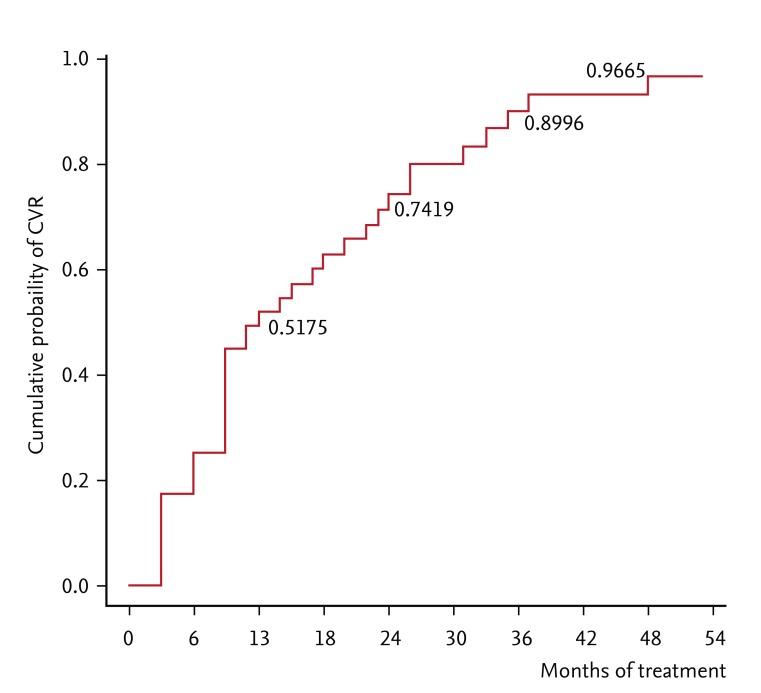
The cumulative probabilities of achieving CVR were 17.3%, 25.0%, 51.8%, 74.2%, and 96.7% at 3, 6, 12, 24, and 48 months of treatment, respectively (Fig. 1). No patient had a primary nonresponse. Six patients experienced viral BT during TDF treatment; three had poor drug compliance, and one patient was a renal transplant recipient receiving immunosuppressive therapy. Following viral BT, the viral load declined below the previous nadir either spontaneously or with good compliance to TDF treatment in all patients.
Virological response predictors
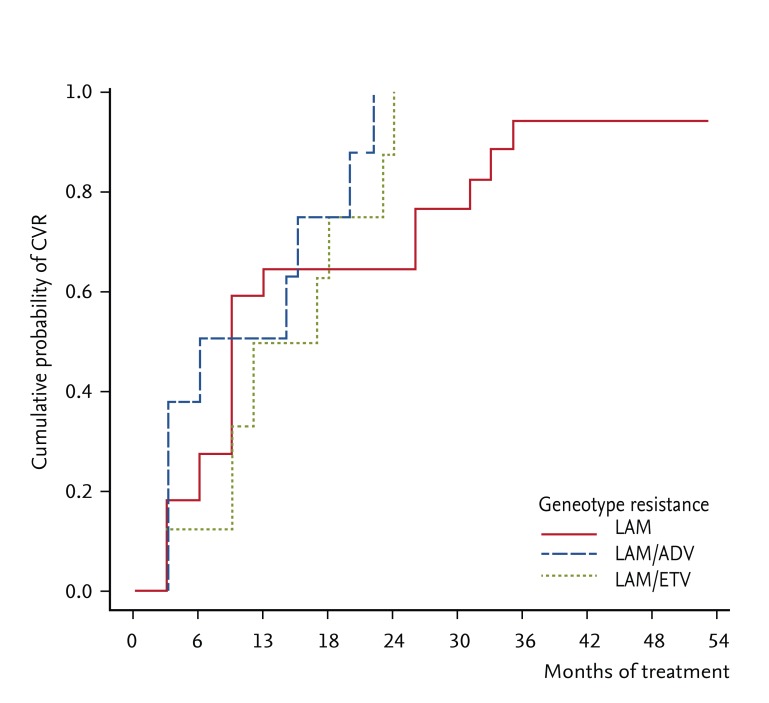
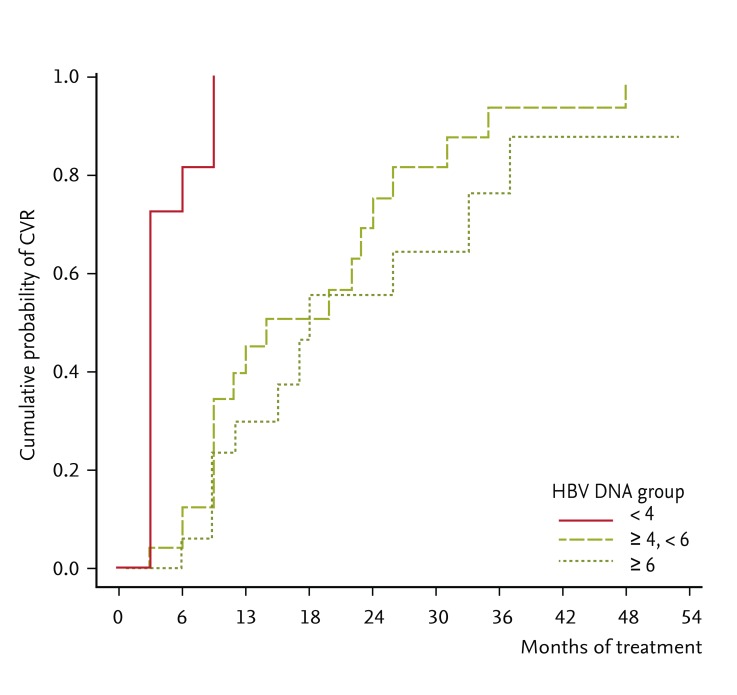
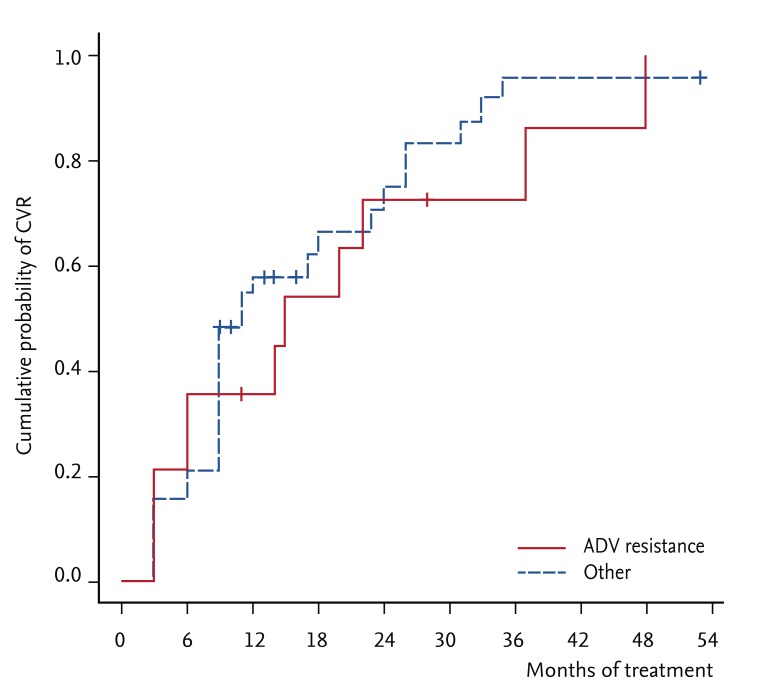
Age, gender, serum ALT levels, HBeAg status at baseline, prior exposure to NAs and treatment duration with prior NAs had no influence on CVR rates (data not shown). The presence of genotypic resistance to LAM, LAM/ADV, or LAM/ETV was not related to the achievement of CVR (p = 0.25) (Fig. 2). Additionally, the HBsAg titer at baseline was not associated with the CVR rate (p = 0.50). However, the HBV DNA level at baseline correlated well with the CVR rate (p = 0.001). When patients were categorized into three groups according to HBV DNA levels at baseline (2 to 4, 4 to 6, and ≥ 6 log IU/mL), lower HBV DNA levels were significantly associated with increased CVR rates (p < 0.001) (Fig. 3). Within the ADV-resistant subgroup of patients, the baseline HBV DNA levels (2 to 4, 4 to 6, and ≥ 6 log IU/mL) also significantly influenced the probability of CVR (p = 0.001).
Efficacy of TDF monotherapy versus combination therapy with LAM or ETV
The efficacy between TDF monotherapy and TDF combination therapy with LAM or ETV did not differ (n = 17 and 35, respectively; p = 0.51) (Fig. 4). Among 22 patients with genotypic resistance against LAM, TDF monotherapy versus LAM or ETV combination therapy did not affect the CVR rates (p = 0.67). In patients with LAM/ADV resistance (n = 8), the CVR rates were not significantly different between TDF monotherapy and LAM or ETV combination therapy (p = 0.87). Similarly, among 16 patients with genotypic resistance against LAM/ETV, CVR rates were similar between TDF plus ETV combination therapy and TDF monotherapy (p = 0.84). Two patients had genotypic resistance to LAM/ADV/ETV, and one reached a CVR 6 months after TDF plus LAM combination therapy. Although another patient who was treat ed with TDF plus ETV did not reach a CVR until 28 months, serum HBV DNA levels declined from 6.83 to 2.31 log IU/mL.
Biochemical and serological responses
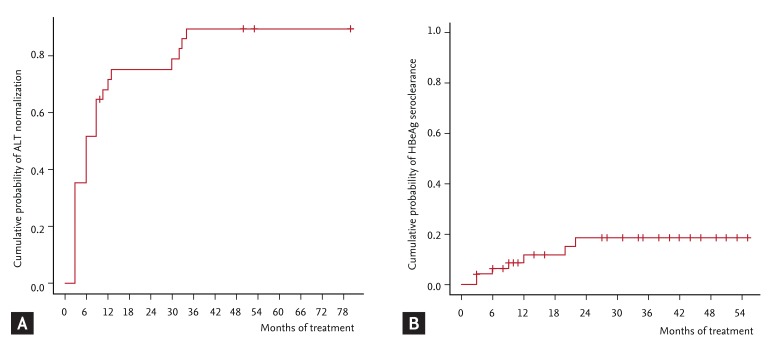
During TDF treatment, ALT levels were normalized in 27 of 31 patients (87.1%) who had elevated ALT at baseline. The probability of ALT normalization was 51.6% at 6 months and 71.6% at 12 months (Fig. 5A). Among 48 HBeAg-positive patients at baseline, HBeAg seroclearance occurred in seven patients (14.6%) after a median duration of 24.5 months (range, 3 to 55). HBeAg seroclearance rates were 6.3% and 11.8% at 6 and 12 months, respectively (Fig. 5B).
Adverse events
No patient developed clinically significant adverse events, such as hepatic decompensation or HCC, during TDF therapy. Additionally, renal toxicity (defined as an increase of 0.5 mg/dL in the serum creatinine level) was not observed. In one patient, the serum phosphorus level decreased from 2.8 to 1.8 mg/dL following 6 months of TDF therapy. This patient had previously experienced symptomatic hypophosphatemia after 59 months of ADV therapy and suffered from muscle weakness and pain during TDF therapy. He discontinued TDF therapy and switched to ETV therapy. Two months after TDF discontinuation, the hypophosphatemia-related symptoms disappeared.
DISCUSSION
In this study, TDF rescue therapy showed a potent antiviral response in CHB patients with multiple previous failures to NA treatment. The cumulative probabilities of achieving CVR were 25% at 6 months, 51.8% at 12 months, 74.2% at 24 months, and 96.7% at 48 months. The HBV DNA level at baseline was the only predictor for treatment efficacy of TDF. The CVR rate was not affected by either TDF monotherapy or combination therapy with LAM or ETV, or by mutations associated with resistance to NAs.
To date, several papers have reported the efficacy of TDF for the treatment of HBV infection refractory to NAs. TDF showed excellent antiviral activity against LAM-resistant HBV independently of the resistance mutation profile in vitro [22]. In patients with LAM-resistant CHB, TDF therapy resulted in a median HBV DNA level decline of 4.5 log copies/mL after median treatment duration of 12 months [23]. In a retrospective study involving 53 LAM-resistant patients, the HBV DNA level after 48 weeks was less than 105 copies/mL in 100% of patients in the TDF group but only in 44% of patients in the ADV group [24]. TDF alone, or combined with LAM, exerted a greater viral reduction than did ADV in LAM-resistant HBV infection without developing phenotypic resistance [25,26]. Similarly, in the present study, TDF showed potent antiviral activity against LAM-resistant HBV. Mutations associated with resistance to LAM were detected in 22 patients, 19 of whom (86.4%) reached a CVR after a median treatment of 9 months (range, 3 to 53).
Patterson et al. [18] reported a 64% CVR rate after 96 weeks of TDF rescue therapy in CHB patients following failures of both LAM and ADV treatments. In that study, 21 of 60 patients had baseline ADV resistance (14 patients with the rtA181T/V mutation and seven patients with the rtN236T mutation), and the authors concluded that the viral response was independent of mutations conferring ADV resistance. In the present study, 14 patients had genotypic resistance to ADV. The probability of reaching a CVR was 35.7%, 72.4%, and 86.2% at 6, 24, and 48 months, respectively. In ADV-resistant patients, the response to TDF was additionally calculated for those with high HBV DNA levels (≥ 4 log IU/mL) at baseline; the CVR rates were 10%, 61.4%, and 80.7% at 6, 24, and 48 months, respectively. Resistance to ADV did not influence CVR during the treatment period (p = 0.57) (Fig. 6). However, in another study, the presence of ADV resistance decreased the efficacy of TDF. The probability of achieving HBV DNA levels below 400 copies/mL was 52% for patients with ADV-resistant variants and 100% for those without ADV-resistant variants [19]. In that study, the mean baseline HBV DNA levels in ADV-resistant patients were more than 2 log IU/mL higher than those in our patients (8.4 log IU/mL vs. 5.6 log IU/mL). The higher levels of baseline HBV DNA may have contributed to the reduced efficacy of TDF therapy in ADV-resistant patients in the previous study. Nevertheless, in vitro studies have found that ADV-resistant variants, including alanine to valine or threonine substitution at position 181 (rtA181V/T) or asparagine to threonine substitution at position 236 (rtN236T), had 3- to 4-fold reduced susceptibility to TDF [27,28]. Thus, the possibility of an altered response to TDF in CHB patients with genotypic resistance to ADV should be considered, especially for those with high baseline HBV DNA levels.
The present study included 40 patients who had failed prior ETV treatment with or without LAM and ADV treatments. Among them, 18 patients showed genotypic resistance to ETV. TDF therapy induced undetectable HBV DNA levels in 49.1% and 89.8% of genotypic ETV-resistant patients at 12 and 24 months, respectively. A retrospective multicenter study conducted by van Bommel et al. [19] included three patients with ETV therapy failure; two with previous ETV treatment and one with sequential LAM and ETV treatments. In one case of genotypic resistance to ETV, the patient showed an immediate response to TDF, and the HBV DNA level was reduced to < 400 copies/mL after 12 weeks. In another study, TDF added to ETV therapy was evaluated as a rescue strategy in 57 CHB patients with multidrug resistance or prior partial response [29]. Four patients with genotypic resistance to ETV showed undetectable levels of HBV DNA after 3 to 9 months, and the presence of genotypic resistance to ETV did not significantly reduce the time to HBV DNA negativity. Although data regarding the role of TDF treatment in CHB patients with treatment failure to ETV are limited, these results along with ours suggest that TDF retains strong activity against HBV in patients with ETV resistance.
In the present study, the HBV DNA level at baseline was the only predictor of CVR achievement. Van Bommel et al. [19] reported that ADV-resistant patients with low HBV DNA levels had a higher chance of responding to TDF monotherapy compared with patients with high HBV DNA levels. In another prospective study that assessed the effectiveness of TDF therapy in 60 CHB patients also showed that persistent viral replication > 15 IU/mL was associated with a higher baseline viral load at all time points until week 96 [18]. Thus, these findings support that the HBV DNA level at the time of switching to TDF is the most important factor for determining the virological response.
Generally, drug combination therapy without cross-resistance is recommended to delay or prevent the emergence of drug-resistant mutants [1,2,30]. For example, current guidelines recommend combination treatment with LAM or ETV for patients who failed to respond to LAM and ADV therapies. However, in this study, the treatment efficacy did not differ between TDF alone and LAM or ETV combination treatment across the patient subgroups resistant to LAM, LAM/ADV and LAM/ETV. Additionally, van Bommel et al. [19] reported that TDF monotherapy was effective without viral BT in a long-term (up to 5 years) follow-up study. However, in a recent study, the viral load reduction was greater in the TDF plus LAM combination therapy group compared with the TDF monotherapy group, ADV monotherapy group and ADV plus LAM combination therapy group [25]. Moreover, reduced sensitivity to TDF was demonstrated in ADV-resistant patients, indicating potential cross-resistance [19,27,28]. Therefore, due to controversies and the small sample size in this study, the necessity for TDF combination therapy cannot be determined currently, especially when considering the associated cost and potential adverse effects. Further research is necessary to explore this issue.
In this study, hypophosphatemia associated with TDF therapy was reported in one patient who had already experienced hypophosphatemia with previous long-term ADV therapy. This report highlights the importance of carefully monitoring serum phosphate levels during TDF therapy for adverse effects, especially in patients who had already experienced ADV-related adverse events or received long-term ADV treatment.
Although the HBV genotype could be a factor affecting the treatment efficacy of antiviral agents, we did not perform genotypic analysis. However, previous studies have shown that almost all HBV-infected patients (98% to 100%) in Korea are of genotype C [31,32,33]. Therefore these results could be applied to our study patients and represent genotype C HBV-infected patients.
In conclusion, TDF used in monotherapy or in combination with other NAs is effective and safe for CHB patients with multiple NA failures during prior treatments. Additionally, the HBV DNA level when switching to TDF is the most important factor for determining the virological response. Optimal TDF therapy regimens according to the presence of mutation profiles should be investigated in future studies.
KEY MESSAGE
Tenofovir disoproxil fumarate (TDF) rescue therapy is effective and safe for chronic hepatitis B patients with prior multiple nucleos(t)ide analogues treatment failure.
Hepatitis B virus DNA level at the time of switch to TDF is the most important factor for determining virologic response.
Further research is necessary to investigate optimal TDF therapy regimens according to the genotypic resistance profiles.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





