


INTRODUCTION
Numerous studies have shown that intravascular ultrasound (IVUS)-guided percutaneous coronary intervention (PCI) decreases the frequency of major adverse cardiac events (MACEs) and stent thrombosis (ST), mainly in patients with stable coronary artery disease undergoing elective PCI [1-4]. However, in the setting of acute myocardial infarction (AMI), the benefits of IVUS guidance during PCI remain a matter of debate [5,6].
Drug-eluting stents (DESs) are a highly efficacious treatment for patients with coronary artery disease, markedly inhibiting neointimal hyperplasia [7-9], and they have demonstrated favorable clinical outcomes even in patients with high-risk clinical conditions such as AMI and diabetes [10]. However, there are also safety concerns about their use in AMI patients, because of an increased risk of ST [11].
Although bare metal stents (BMSs) are less effective than DESs for inhibiting neointimal proliferation [8,9], they are associated with similar clinical outcomes when adequate stent expansion can be achieved during an index procedure [12-14]. Furthermore, a recent meta-analysis in primary angioplasty reported that BMSs were not associated with an increased risk of very late ST [15]. Thus, we hypothesized that IVUS-guided PCI using BMSs would show similar efficacy and better safety at long-term follow-up than IVUS-guided DES implantation in AMI patients undergoing primary PCI.
METHODS
We analyzed data retrospectively from patients with ST-segment elevation myocardial infarction (STEMI) who underwent primary PCI for a de novo culprit lesion from January 2000 to July 2008.
During primary PCI, BMSs were used exclusively from January 2000 to May 2003, whereas DESs were implanted exclusively from June 2003 to July 2008. Regardless of stent type, all procedures were performed according to standard techniques via the femoral approach.
All patients were older than 18 years. To be eligible for primary PCI, patients had to meet the following criteria: symptoms present < 12 hours from onset to time of hospital arrival, and ST-segment elevation or a new left bundle branch block. All interventions were performed according to current standard guidelines. Procedural success in the infarct-related artery was defined as residual stenosis < 30% by visual estimation with thrombolysis in myocardial infarction (TIMI) grade 3 flow. Patients were excluded if they had: intolerance or a contraindication to aspirin or thienopyridine, advanced heart failure or an ejection fraction < 30%, or another severe comorbidity. The patients were premedicated with aspirin 300 mg, which was continued indefinitely, and given a loading dose of ticlopidine (500 mg) or clopidogrel (300 to 600 mg) before PCI. The patients were advised to stay on dual antiplatelet therapy for a minimum of 3 months in cases of BMS and 12 months for DES.
IVUS (Atlantis, Boston Scientific Corp., Minneapolis, MN, USA) was performed and interpreted by the physician. IVUS images were obtained after administration of 200 mcg of nitroglycerin. After preinterventional or post-ballooning IVUS was performed, stent size and diameter were determined according to IVUS parameters. When postdilation was required to optimize stent expansion or apposition, a balloon shorter than the stent length was used with careful positioning of the balloon inside the stent to avoid injury at the edge. Stent underexpansion was defined as minimal stent area (MSA) < 6.5 mm2 for BMS and 5.0 mm2 for DES [16]. Coronary angiography results were analyzed using a computer-assisted system for quantitative coronary angiography (QCA) analysis (Digital Cardiac Imaging System, Philips Medical Systems, Best, The Netherlands) using end diastolic frames and a contrast-filled guiding catheter for calibration. The percent diameter stenosis was defined as [1 - (minimal lumen diameter/reference vessel diameter)] ├Ś 100.
The primary endpoint was defined as the incidence of MACEs including all cause death, myocardial infarction (MI), target vessel revascularization (TVR), and ST at 3-year follow-up. MI was defined as an elevation in creatinine kinase-MB Ōēź 3 times the upper normal value. TVR was defined as percutaneous or surgical revascularization of the stented vessel. ST was defined using the Academic Research Consortium definition [17].
Statistical analysis
Statistical analyses were performed using the SPSS software version 15.0 (SPSS Inc., Chicago, IL, USA). Continuous data are presented as means ┬▒ standard deviation while categorical data are presented as frequencies. Continuous variables were compared using unpaired Student t tests. Categorical variables were compared using chi-square and Fisher exact tests. The cumulative incidence of MACE was estimated according to the Kaplan-Meier method, and curves were compared using the log-rank test. Cox multivariate regression analyses were used to determine predictors of cardiac events. Variables with p < 0.10 on univariate analysis and classical risk factors such as age, gender, diabetes, hypertension, and hyperlipidemia, were entered into a multivariate regression analysis. These p values < 0.05 were considered to indicate statistical significance.
RESULTS
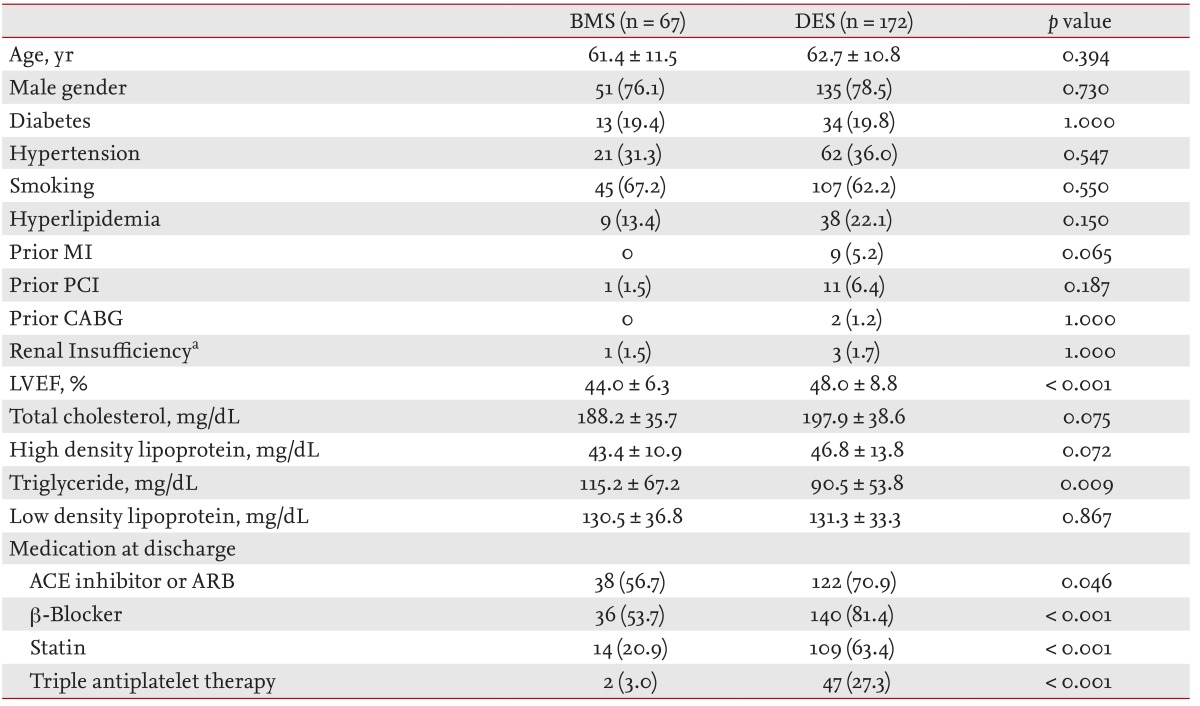
In total, 337 patients who underwent primary PCI with BMS (107 patients) or DES (230 patients) implantation were enrolled consecutively. In total, 239 STEMI patients received BMS (67 patients with 77 stents) or DES (172 patients with 221 stents) under IVUS guidance (Fig. 1). During enrollment, four types of DES were used: sirolimus-eluting stents (SESs, 48.3%; Cypher, Cordis, Miami Lakes, FL, USA), paclitaxel-eluting stents (PESs, 29.0%; Taxus, Boston Scientif ic, Natick, MA, USA), zotarolimus-eluting stents (ZESs, 16.9%; Endeavor Sprint, Medtronic CardioVascular, Santa Rosa, CA, USA), and everolimus-eluting stents (EESs, 5.8%; Xience V, Abbott Vascular Devices, Santa Clara, CA, USA). Patients undergoing IVUS-guided BMS implantation had decreased left ventricular ejection fraction (p < 0.001). The frequency of diabetes mellitus and hypertension did not differ between the groups (Table 1). Procedural characteristics are presented in Table 2. Infarct-related arteries and lesion type, by American College of Cardiology/American Heart Association classification, were similar between the DES and BMS groups. However, the presence of intracoronary thrombus by coronary angiography and performance of thrombus aspiration were significantly higher in the BMS group than the DES group (73.1% vs. 51.7%, p = 0.010; and 35.8% vs. 8.7%, p < 0.001, respectively). The reference vessel diameter and stent diameter were significantly larger in the BMS group than in the DES group (3.47 ┬▒ 0.43 mm vs. 3.23 ┬▒ 0.40 mm and 3.58 ┬▒ 0.42 mm vs. 3.23 ┬▒ 0.39 mm; all p < 0.05). Lesion length and stent length were longer in the DES group (28.5 ┬▒ 14.2 mm vs. 23.8 ┬▒ 11.7 mm and 32.0 ┬▒ 15.4 mm vs. 26.9 ┬▒ 12.5 mm; both p < 0.01). The minimal stent diameter by QCA and MSA by IVUS were significantly larger in the BMS group than the DES group (3.31 ┬▒ 0.44 mm vs. 2.89 ┬▒ 0.39 mm and 7.51 ┬▒ 2.15 mm2 vs. 6.57 ┬▒ 2.16 mm2; both p < 0.05) (Table 3). However, the incidence of stent underexpansion was higher in the BMS group (37.3% vs. 22.1%; p = 0.023). Prescriptions of ╬▓ blockers, angiotensin converting enzyme inhibitors or angiotensin receptor blockers, statins, and triple antiplatelet therapy were more frequent in the DES group (all p < 0.05).
Clinical outcomes
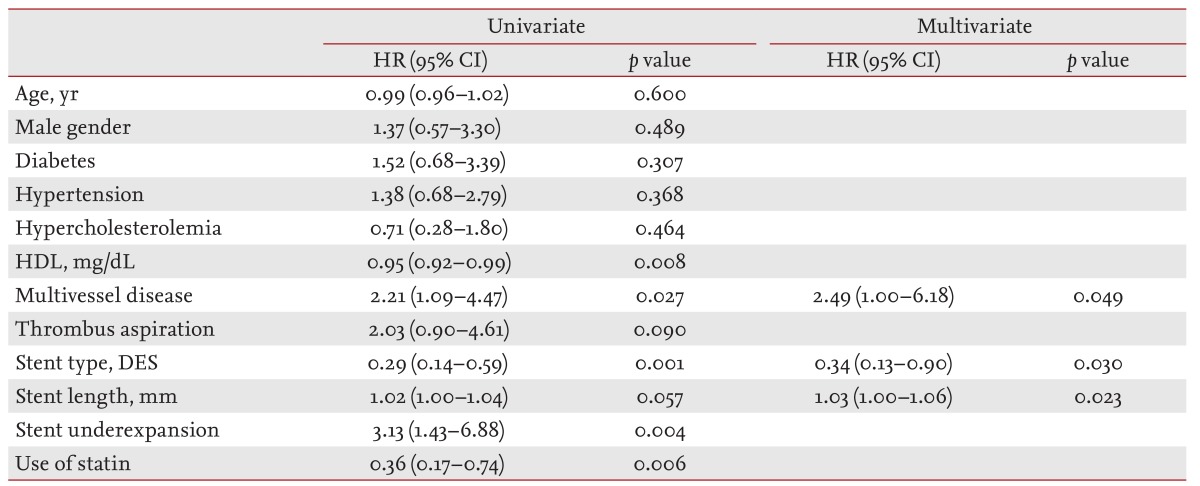
All patients were followed-up with face to face contact or by telephone and more than half of patients received angiographic follow-up examinations in each group (53.7% of BMS and 61.0% of DES). There was no difference in all cause mortality or MI between the DES and BMS groups at 1-, 2-, and 3-year follow-up (Table 4). However, the incidence of TVR was significantly lower in the DES group than the BMS group (6.4% vs. 17.9%, p = 0.006 at 1 year; 8.1% vs. 23.9%, p = 0.002 at 2 years; and 9.3% vs. 23.9%, p = 0.005 at 3 years, respectively). However, the incidence of TVR did not differ among the four DES types (8.6% of SES, 10.0% of PES, 14.3% of ZES, and 0% of EES, p = 0.736 at 3 years). The cumulative incidence of MACE was significantly lower in the DES group (7.6% vs. 22.4%, p = 0.003 at 1 year; 9.3% vs. 29.9%, p < 0.001 at 2 years; and 11.0% vs. 29.9%, p = 0.001 at 3 years, respectively). The incidence of definite or probable ST did not differ between the groups (1.7% vs. 1.5%, p = 1.0 at 1 and 2 years; 2.3% vs. 1.5%, p = 1.0 at 3 years, respectively). These clinical outcomes were seen at the time of the 1-year follow-up and were sustained during 3 years of follow-up. On univariate analysis, stent type, stent underexpansion, high density lipoprotein level, multivessel disease and the prescription of statin were associated with 3-year MACE. After adjustment for these parameters, IVUS-guided DES implantation was associated with a lower rate of 3-year MACE (hazard ratio [HR], 0.34; 95% confidence interval [CI], 0.13 to 0.90; p = 0.030) versus BMS. In addition, stent length (HR, 1.03; 95% CI, 1.00 to 1.06; p = 0.023) and multivessel disease (HR, 2.49; 95% CI, 1.00 to 6.18; p = 0.049) were independent predictors of 3-year MACE (Table 5).
DISCUSSION
The major finding of the present study was that despite the fact that IVUS-guided BMS implantation was associated with significantly larger MSA after stenting, IVUS-guided DES implantation showed better efficacy by diminishing the rate of TVR with similar safety and no increased risk of ST up to 3 years. In addition, IVUS-guided BMS versus DES implantation in patients with STEMI undergoing primary PCI showed similar long-term clinical outcomes to those seen in patients with stable coronary artery stenosis.
Because DESs have proven effective for inhibiting intimal hyperplasia in stable coronary lesions [9], STEMI has been treated with DESs [18-22]. Despite concerns regarding an increased risk of ST due to delayed healing [11], numerous studies have reported superior efficacy with DES versus BMS, driven mainly by reduced TVR or target lesion revascularization (TLR), without safety issues, in AMI patients during 3 to 5 years of follow-up [18-22]. A recent optical coherence tomography substudy of the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZON-AMI) trial demonstrated that most struts (> 94%) were covered in PES at 13-month follow-up, suggesting that the risk of ST may not be as high as previously anticipated, compared to BMS [23]. Our results are consistent with these findings. However, a recent meta-analysis of 13 randomized trials in primary angioplasty showed that although first-generation DES compared to BMS yielded a significantly lower incidence of TVR (12.7% vs. 20.1%; HR, 0.57; 95% CI, 0.50 to 0.66; p < 0.001) with no effect on mortality, reinfarction, or ST, the risk of very late ST and late infarction were significantly higher in patients treated with DES (HR, 2.81; 95% CI, 1.28 to 6.19; p = 0.04 and HR, 2.06; 95% CI, 1.22 to 3.49; p = 0.03, respectively) [15]. Taken together, DES safety may still be inconclusive in AMI patients although longterm efficacy seems to be favorable for DES. Thus, larger populations with longer-term follow-up will be necessary to clarify this issue in the setting of AMI.
Although BMS showed less inhibition of neointimal hyperplasia than DES, adequate BMS expansion with or without IVUS guidance provided favorable clinical outcomes, similar to those for DES [12]. Furthermore, the benefit of DES use was limited to vessels Ōēż 3 mm in size [13,24]. In the A Randomized Controlled Trial of Angiography versus Intravascular Ultrasound-Directed Bare Metal Coronary Stent Placement (AVID) trial, the final MSA was 7.55 ┬▒ 2.82 mm2 in the IVUS-guided group and 12-month TLR was only 8.1% in 394 patients receiving elective BMS placement [12]. In the present study, the IVUS-guided BMS group had vessel sizes > 3 mm and a similar final MSA to the AVID trial, predicting that long-term clinical outcomes were comparable with those in the IVUS-guided DES group. However, IVUS-guided DES implantation showed a lower incidence of MACE at 3-year follow-up, driven primarily by a reduced TVR rate, suggesting that IVUS-guided BMS versus DES implantation in patients with STEMI undergoing primary PCI had similar long-term clinical outcomes to those seen in stable coronary artery stenosis [9,24].
STEMI has been considered an off-label DES use [25]. Moreover, several studies demonstrated that STEMI is a strong predictor for the development of early or late ST [26,27]. The incidence of ST after DES implantation has been reported to be 3% to 5% of patients with STEMI undergoing primary PCI [19-22]. Because of large thrombotic burden and a higher chance of incompletely apposed struts in STEMI patients, the use of DES has a potential risk of ST and consequently adverse cardiac events. However, the present study showed a relatively low incidence (2.3%) of ST compared to previous studies [19-22]. A possible explanation is that with either BMS or DES, implantation under IVUS guidance might contribute to reducing the rate of ST.
In a previous study, we demonstrated that IVUS-guided PCI may reduce long-term mortality compared to angiography-guided PCI in real world practice [2], consistent with a study on unprotected left mains [3]. In these studies, 50% to 60% of the study population was diagnosed with acute coronary syndrome. Another study by Roy et al. [4] showed that IVUS-guided PCI significantly reduced the development of subacute ST after DES implantation.
The benefits of IVUS-guided PCI seem to be offset by AMI presentation. Because the number of treated lesions and stent implantation were both higher and procedural time was prolonged in the IVUS-guided group, 1-year clinical outcomes did not dif fer between IVUS-guided PCI and angiography-guided PCI [5,6]. Whether the impact of IVUS-guided PCI is different depends on clinical presentation and a randomized clinical trial is needed.
This retrospective study has several limitations. First, the chronological difference between the use of BMS and DES and the fact that the decision for IVUS guidance during primary PCI was at the physician's discretion may have introduced selection bias. Second, although we evaluated predictors of MACE performing multivariate analysis, unmeasured confounders could affect the clinical results. Third, because few patients were treated with BMS or DES under IVUS guidance, the clinical events during 3 years of follow-up may be underestimated. The study was also underpowered to detect rarely occurring events, such as ST. Fourth, our finding that the use of DES under IVUS guidance showed better efficacy with no increased risk of ST was similar to that in other subsets of lesions or patients. Thus, the clinical implications of our results may be limited. Finally, a heterogeneous baseline, procedural characteristics, and medication patterns between BMS and DES patients might affect long-term outcomes. In fact, recent DES trials have included more complex lesions and/or high-risk patients compared to previous BMS studies, accounting for the differences between baseline characteristics and medication patterns.
Although in the present study IVUS-guided BMS implantation was associated with a larger final MSA, IVUS-guided DES implantation appeared to be as safe as BMS and showed significant benefits for reducing the risk of TVR for up to 3 years in patients with STEMI undergoing primary PCI.
KEY MESSAGE
1. Even if intravascular ultrasound (IVUS) guidance, drug-eluting stent (DES) implantation in primary percutaneous coronary intervention had better efficacy compared with bare metal stent.
2. IVUS-guided DES implantation showed favorable long-term safety without increased risk of stent thrombosis in the ST-segment elevation myocardial infarction setting.




 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





