


INTRODUCTION
Neurocardiogenic syncope is the most common cause of syncope in patients without underlying disease [1]. Neurocardiogenic syncope has a peak incidence in subjects in their late teens and early twenties [2]. Tilt-table testing (TTT) is used widely to diagnose neurocardiogenic syncope. The positive rate of TTT with or without a history of syncope ranges from 23.8 to 74% [3-6]. Many researchers have studied treatments of neurocardiogenic syncope including salt intake [7], physical maneuvers [8,9], beta-blockers [10,11], midodrine [12], fludrocortisones [13], paroxetine [14], and cardiac pacing [15]; however, the results are conflicting. In general, the prognosis of patients with neurocardiogenic syncope is benign, although some patients experience not only recurrent syncopal episodes but also serious head injuries despite treatment. Therefore, the identification of high-risk patients is important for treatment and follow-up. The frequency of previous syncopal episodes has been reported to be the most powerful predictor of recurrent neurocardiogenic syncope [16-21]. No other prognostic factors have been confirmed for males in their late teens and early twenties. Therefore, this study sought to identify prognostic factors for neurocardiogenic syncope in males in their late teens and early twenties.
METHODS
Consecutive males with unexplained syncope seen between September 2006 and September 2008 were included. Subjects with underlying disease or abnormal electrocardiograms (ECGs) and those taking any medications were excluded. Abnormal ECGs included rhythms other than sinus rhythm, right- or left-axis deviation, left- or right-ventricular hypertrophy, Mobitz type 2 second-degree atrioventricular block, complete atrioventricular block, left bundle-branch block, and pathological Q-wave and abnormal ST-segment or T-wave changes.
TTT was performed according to the Italian protocol [22,23]. The subjects fasted for at least 3 hours before the test. The subjects were monitored throughout testing with 3-lead electrocardiography and automated blood pressure cuff measurements every 2 minutes. The TTT consisted of passive and drug-provocation phases. After a 5-minute rest in the supine position, the subjects were tilted head-up to a 70° angle on the table for 30 minutes during the passive phase. If the passive phase was negative, the subjects were given sublingual nitroglycerin (0.4 mg) and tilted to the same angle for another 20 minutes during the drug-provocation phase. The endpoint of the TTT was the induction of syncope with significant hypotension. Positive results were classified into the following three types [22,24]: type 1 (mixed) was defined as hypotension and heart rate 40-60/minutes; type 2 (cardioinhibitory) was defined as heart rate < 40/minutes or asystole for ≥ 3 seconds; and type 3 (vasodepressor) was defined as pure hypotension without bradycardia. Hypotension was defined as decreased blood pressure causing syncope or signs of poor tissue perfusion. The subjects with positive results were educated on the prevention of syncope, including the avoidance of predisposing factors, lying down at the onset of prodromal symptoms, fluid or salt intake, and physical maneuvers. No medications were prescribed for subjects with positive results. The subjects were followed in the outpatient clinic or by telephone on a regular basis for 12 months. All subjects provided informed consent.
Statistical analysis
We analyzed the frequency of previous syncope, the TTT phase that gave a positive result, the TTT duration until a positive result, the types of neurocardiogenic syncope, and the recurrence rate of syncope during the follow-up period. The results are expressed as the mean ± SD or median (interquartile range, IQR) for data that were not distributed normally. The Mann-Whitney U test and Kruskal-Wallis test were used for statistical analysis of data that were not distributed normally. Univariate and multivariate logistic regression analyses were used to identify variables associated with the recurrence of syncope during the follow-up period. A p value < 0.05 was considered significant. The data were analyzed with the SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
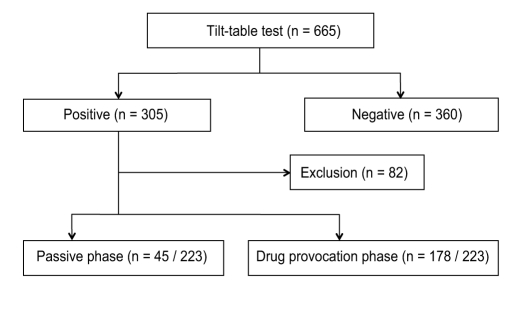
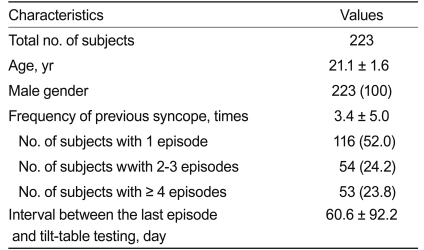
Of the 665 male subjects (mean age, 22.0 years; range, 17 to 27) who underwent testing, 305 (45.8%) had positive results on TTT. Of the subjects with positive results, 82 were excluded because of abnormal ECGs or loss to follow-up (Fig. 1). We followed 223 subjects (mean age, 21.1 years; range, 18 to 26) for 12 months. The frequency of previous syncopal episodes was 3.4 ± 5.0 (Table 1).
Tilt-table test and follow-up results
There were 45 (20.2%) subjects with positive results during the passive phase and 178 (79.8%) during the drug-provocation phase (Fig. 1). There were 146 (65.5%), 39 (17.5%), and 38 (17.0%) type 1 to 3 subjects, respectively. Syncope recurred in 67 (30.0%) subjects. The frequency of recurrence of syncopal episodes during the follow-up period was 1.3 ± 2.4. No recurrences occurred in 95 of 116 subjects (81.9%) with one previous syncopal episode, 36 of 54 subjects (66.7%) with two or three syncopal episodes, and 25 of 53 subjects (47.2%) with four or more syncopal episodes.
Factors related to the recurrence of syncope
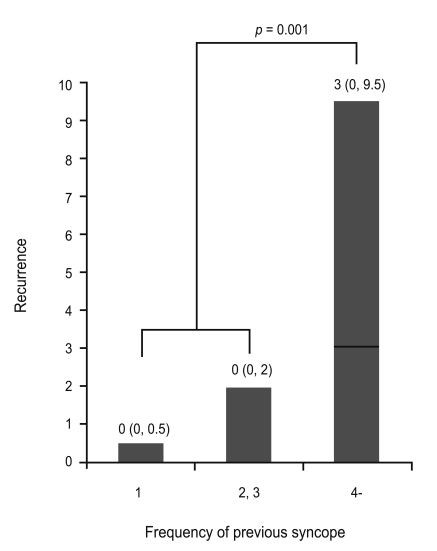
The subjects with four or more previous syncopal episodes in their lifetime had significantly more recurrences of syncopal episodes than did those with fewer than four (1, 2-3, and ≥ 4; 0 [IQR, 0 to 0.5], 0 [IQR, 0 to 2], and 3 [IQR, 0 to 9.5], respectively; p = 0.001) (Fig. 2). The subjects with positive results during the passive phase had significantly more recurrences of syncope than did those with positive results only during the drug-provocation phase (1 [IQR, 0 to 4] and 0 [IQR, 0 to 1], respectively; p = 0.022) (Fig. 3). The subjects (n = 7 of 45) with positive results during the early passive phase (≤ 12 minutes) had significantly more recurrences of syncopal episodes than did subjects (n = 38 of 45) with positive results during the late passive phase (> 12 minutes) (4 [IQR, 3 to 7] and 0 [IQR, 0 to 4], respectively; p = 0.011) (Fig. 3). However, there were no significant differences between the subjects with positive results during the early (≤ 10 minutes, n = 146 of 178) and late (> 10 minutes, n = 32 of 178) drug-provocation phases (0 [IQR, 0 to 2] and 0 [IQR, 0 to 0.5], respectively; p = 0.614) or among the types of neurocardiogenic syncope (types 1 to 3; 0 [IQR, 0 to 1], 0 [IQR, 0 to 3], and 0 [IQR, 0 to 3], respectively; p = 0.435) and the recurrence of syncope. Frequent previous syncopal episodes (≥ 4; p = 0.001) and positive results during the passive phase of TTT (p = 0.001) were significantly associated with the recurrence of syncope (Table 2).
DISCUSSION
This prospective, observational study elucidated prognostic factors for neurocardiogenic syncope in males in their late teens and early twenties in whom the incidence of neurocardiogenic syncope is high [2]. We found that most subjects (81.9%) with one previous syncopal episode had no recurrence and that frequent previous syncopal episodes in their lifetime (≥ 4), a positive result during the passive phase of TTT, and positive results during the early passive phase (≤ 12 minutes) were significantly related to the recurrence rate of syncope. Therefore, a positive result during the early passive phase of TTT and frequent previous syncopal episodes might be prognostic factors for neurocardiogenic syncope in males in their late teens and early twenties.
In previous studies, the frequency of syncope before TTT was the most powerful predictor for recurrent syncope [16-20]. Female gender, a history of bronchial asthma, and the number of previous syncopal episodes may predict recurrences of neurocardiogenic syncope [21]. However, the TTT phase or period associated with positive results as prognostic factors have not been studied in males in their late teens and early twenties.
Neurocardiogenic syncope occurs frequently during prolonged motionless standing, and the passive phase is similar to this situation. The drug-provocation phase is performed on subjects who can tolerate the passive phase. Such subjects were better able to tolerate prolonged motionless standing. Therefore, subjects with a positive result during the passive phase would tend toward a high recurrence rate of syncope. Furthermore, subjects with a positive result during the early passive phase could be more susceptible to a shorter duration of motionless standing.
The classification of neurocardiogenic syncope is based on the results of TTT [22,24]. The mechanisms of each type and the relationship between the type and prognosis are debatable [25].
For patients suspected of neurocardiogenic syncope, it is important to obtain a medical history and to perform TTT. Patients with positive results during the early passive phase of TTT and with more frequent episodes of previous syncope need to be followed closely and treated optimally.
Limitations
The follow-up period of our subjects was relatively short; therefore, future prospective studies are needed to ascertain the recurrence of syncope in more subjects for longer periods of time at various centers. There are different TTT protocols (e.g., the Westminster protocol using isoproterenol for the drug-provocation phase). The Italian protocol with nitroglycerin is comparable to the Westminster protocol with isoproterenol [22,23].


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





