


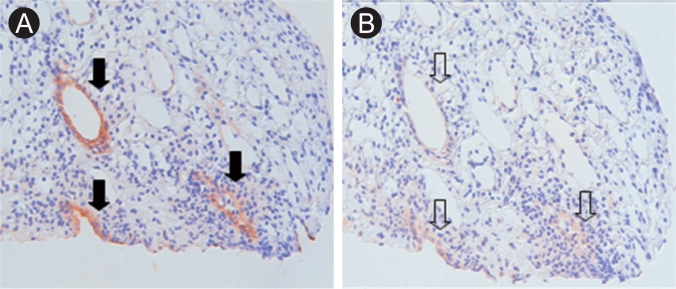
A 44-year-old female was referred to our outpatient clinic with metabolic acidosis and vomiting. She had a history of toxic hepatitis, but no medications. On admission, her blood pressure was 120/70 mmHg with a pulse of 68 beats/min. The laboratory findings showed normal anion gap metabolic acidosis: Na 140 mmol/L, K 1.4 mmol/L, Cl 113 mmol/L, pH 7.192, and bicarbonate 12 mmol/L. The urine chemistry was pH 7.0, Na 55 mmol/L, K 14 mmol/L, and Cl 63 mmol/L (hyperchloremic metabolic acidosis of renal origin). Abdominal computed tomography revealed medullary nephrocalcinosis (Fig. 1). The renal pathology was non-specific. There was decreased net H+ secretion in the collecting tubules, resulting in a high urine pH. Acidification in the collecting tubules is primarily achieved via H secretion by luminal H+-ATPase. However, immunostaining for H+-ATPase was negative (Fig. 2). After alkali replacement with sodium bicarbonate, the serum bicarbonate recovered to above the lower normal limit (26.6 mmol/L). She was discharged in an improved condition.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |