


INTRODUCTION
The identification of a subepithelial lesion during endoscopy is a frequent occurrence. Subepithelial lesions consist of a diverse group of distinct histologic diagnoses ranging from benign to premalignant and malignant. When endoscopic ultrasonography (EUS) came into use, the hope was that benign and malignant subepithelial lesions could be easily distinguished on the basis of their endosonographic characteristics [1]. However, the specificity of EUS imaging findings alone has been disappointing [2], and tissue acquisition and pathologic confirmation are usually required for a specific diagnosis.
Endoscopic biopsies with forceps rarely provide a diagnosis because lesions in the submucosa are beyond the reach of conventional-sized forceps [3,4]. For this reason, jumbo biopsy, EUS-guided fine needle aspiration (EUS-FNA), and endoscopic submucosal resection (ESMR) have been attempted. However, these procedures have many limitations such as lack of histology, low diagnostic yields, relatively high complication rates, and the need for additional diagnostic procedures. Therefore, we sought to determine prospectively the diagnostic yield of tissue sampling using the bite-on-bite technique with conventional-sized forceps for incidental subepithelial lesions during diagnostic endoscopy.
MATERIALS AND METHODS
Patients
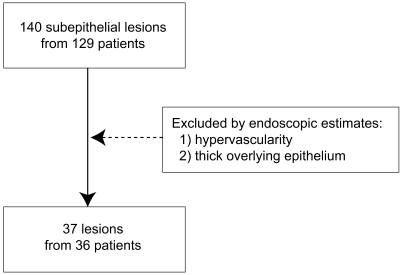
One hundred and forty submucosal lesions were identified in 129 patients during conventional diagnostic esophagogastroduodenoscopy by one examiner from October 2003 to November 2004. During the examination of 36 of these patients (15 women, 21 men; mean age 54 years; age range 26-72 years), bite-on-bite biopsies with conventional-sized forceps (FB-25K-1; Olympus, Tokyo, Japan) were taken for 37 lesions not determined to be hypervascular or to have a thick overlying epithelium (Fig. 1). Mucosae were considered hypervascular based on the presence of vascular engorgement, telangiectasia, or prominent vessels. The thickness of the overlying epithelium was assessed using the degree of epithelial transparency and the thickness of the bridging fold.
Methods
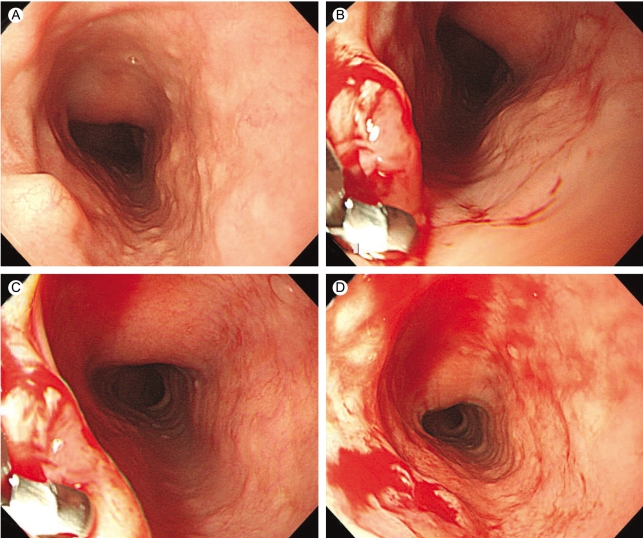
All patients underwent routine upper endoscopy (GIF Q240X; Olympus). Two to eight bites per lesion were performed to obtain submucosal tissue. The bites were performed using the bite-on-bite technique in which each bite is directly on top of the previous one in an attempt to burrow into the lesion (Fig. 2). All procedures were performed by a single experienced endoscopist. Diagnostic yields were calculated as a function of location and size of lesion.
The study was approved by our institutional ethical committee and written informed consent was obtained from each patient.
RESULTS
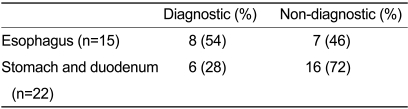
The bite-on-bite technique was diagnostic in 14 of the 37 lesions (38%) (Table 1) including eight of 15 esophageal subepithelial lesions. Seven of the eight esophageal lesions were leiomyomas and one was a granular cell tumor. The technique was diagnostic in four of 16 gastric subepithelial lesions, a lymphangioma, a case of ectopic pancreas tissue, a gastrointestinal stromal tumor, and a leiomyoma, and in two of six duodenal subepithelial lesions, both of which were lipomas. The diagnostic yield for the esophagus was 54% and that for the stomach and duodenum was 28% (Table 2). Thus, the diagnostic yield tended to be greater in the esophagus than in the stomach and duodenum (p=0.109).
The diagnostic yield for subepithelial lesions was 33% for those below 1 cm and 46% for those above 1 cm (Table 3). However, the relationship between diagnostic yield and size of the lesion was not significant (p=0.495).
Blood oozing for over 30 sec occurred in five cases (14%), each of which was easily controlled by dilute epinephrine injection (1:10000, 2 cases) or hemoclip (3 cases). No delayed complications occurred.
DISCUSSION
Subepithelial lesions represent a spectrum of histologic lesions located beneath the mucosal lining of the gastrointestinal tract. Most of these lesions do not cause symptoms and are found incidentally during radiographic or endoscopic examinations [5]. They are located within the true submucosa or may arise from the muscularis propria. Subepithelial lesions are relatively common findings during upper endoscopy, with an estimated incidence of 0.3% [6]. The majority of tumors in the gastrointestinal tract are leiomyomas [7]. In addition to leiomyomas, fibromas, ectopic pancreatic tissues, lipomas, and granular cell tumors are also observed. A large proportion of submucosal tumors in the gastrointestinal tract are benign, but several malignant submucosal tumors, including leiomyosarcomas and malignant lymphomas, do occur.
Techniques for endoscopic evaluation of gastrointestinal subepithelial lesions include conventional endoscopy, jumbo biopsy, EUS, EUS-FNA, and ESMR. Although traditionally used as a first-line diagnostic procedure for subepithelial lesions, endoscopic biopsy sampling with conventional-sized forceps is frequently non-diagnostic, primarily because of its limited depth of penetration. In fact, less than one-third of forceps biopsies include a significant amount of submucosae [3].
One procedure commonly employed for sampling subepithelial lesions is the use of large-capacity (jumbo) forceps biopsies to perform a bite-on-bite technique. With a large-channel endoscope, the forceps are passed multiple times with each bite directly on top of the previous bite in an attempt to burrow into the lesion. Compared to that of conventional-sized forceps, the use of jumbo forceps may increase the surface area of the tissue sample but does not significantly increase its depth [8]. Also, bleeding as a complication of this technique may be troublesome.
In our study, we used a bite-on-bite technique with conventional-sized forceps and endoscopy instead of jumbo forceps and a large-channel endoscope. Blood oozing over 30 sec occurred in five cases (14%), but was easily controlled with diluted epinephrine injection or a hemoclip because we excluded hypervascular lesions and used conventional-sized forceps.
EUS helps differentiate true subepithelial lesions from extrinsic ones, as well as from large intraluminal and extraluminal vessels. If an intramural lesion is identified, EUS can be used to ascertain the exact size and layer of origin, in addition to additional morphologic features that can suggest a diagnosis [2]. On EUS, the mass can be either homogenous or heterogeneous and can be hyperechoic, hypoechoic, or anechoic. Although some of the lesions have distinctive EUS features, using endosonographic criteria alone appears to be inadequate. Gress et al [9] showed that interobserver agreement among experienced endosonographers was poor in the diagnosis of carcinoids, metastases, and granular cell tumors. In a prospective multicenter study by Rosch et al [10], EUS alone had a sensitivity of 64% and a specificity of 80% in the diagnosis of malignant subepithelial lesions. EUS findings are inadequate for distinguishing benign from malignant stromal cell tumors [11-13]. Hence, to thoroughly characterize a subepithelial lesion and obtain a definite diagnosis, tissue acquisition and pathologic confirmation are generally needed. EUS was not performed in our study. Because incidental subepithelial lesions were immediately biopsied by the bite-on-bite technique during diagnostic endoscopy, additional diagnostic procedures were not required.
EUS-FNA is commonly used to confirm the presence of malignancy in lymph nodes or organs adjacent to the gastrointestinal tract [2]. EUS-FNA can be used to obtain a specimen for cytologic examination, which is useful for distinguishing benign from malignant lesions, but less useful for determining the type of benign lesion. The sensitivity, specificity, and accuracy of cytologic evaluation for intramural lesions are low [14-16].
ESMR is usually reserved for lesions that are confined to the submucosal or mucosal layers due to the increased risk of perforation associated with ESMR for lesions in the muscularis propria. A potential advantage of ESMR is the ability to obtain a larger tissue specimen, which may enhance the diagnostic yield.
In a prospective study by Cantor et al [1], diagnostic yield was greater for ESMR than with jumbo forceps; the diagnostic yield was 17% for jumbo forceps and 87% for ESMR. However, the complications of ESMR, including post-resection bleeding and perforation, can be prohibitive [17]. Cantor et al [1] proposed that ESMR should be performed in symptomatic patients (e.g., patients with dysphagia, anemia, gastrointestinal bleeding, abdominal pain, and lesions that may be obstructive), whereas in asymptomatic patients, it should be limited to lesions that are either malignant or potentially malignant in an effort to reduce the complication rate.
Subepithelial lesions without a definite diagnosis based on EUS and tissue sampling should receive periodic follow-up examination by endoscopy or EUS. The duration of follow-up depends on the degree of suspicion on the part of the examiner that the lesion has malignant potential, as well as on the age and health of the patient [2].
In this study, a bite-on-bite technique with conventional-sized forceps was used. This technique has several benefits. The first is that it is simple and requires no additional diagnostic procedures and/or equipment, including EUS. Hence, it is economical and time-saving. The second is that definite diagnosis is possible by acquiring tissue, so that periodic follow-up examination by endoscopy or EUS is not necessary. A limitation of the technique is that it is not applicable to lesions that are thought to be hypervascular or to have thick overlying epithelium.
The diagnostic rate of esophageal subepithelial lesions in the present study was over 50%. Two possible explanations exist for the apparently higher diagnostic yield for the esophagus compared to that for the stomach and duodenum. First, the epithelium of the esophagus is thinner; second, over 60% of esophageal leiomyomas originate from the muscularis mucosae, while almost all gastric leiomyomas (>90%) originate from the muscularis propria [18]. Therefore, in our opinion, the bite-on-bite technique should be attempted in select cases of esophageal lesions before performing EUS.
In conclusion, bite-on-bite biopsy of subepithelial lesions with conventional-sized forceps is an effective and safe method in select cases. It could be tried for incidental subepithelial lesions, especially in the esophagus during diagnostic endoscopy, unless the lesion has a high risk of bleeding or a thick overlying epithelium. Some subepithelial lesions arising in the lamina propria or muscularis mucosae can be diagnosed by this technique, in which case further imaging is not required.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





