


INTRODUCTION
Ventricular premature complexes (VPCs) are the most common arrhythmias observed in the patients who are without structural heart disease. It has been recently reported that frequent VPCs could evoke left ventricular (LV) dilation, and this might be reversed by suppression of the VPCs1-3). We experienced a patient with severe LV dysfunction, the so-called tachycardiomyopathy, that was induced by very frequent and longstanding VPCs. The LV dilation and dysfunction were completely reversed with performing radiofrequency catheter ablation for eliminating the VPCs, which originated from the right ventricular outflow tract (RVOT).
CASE REPORT
A 32-year-old male patient visited the emergency room and presented with resting dyspnea and palpitations. He had suffered from intermittent palpitations and dyspnea (class II) for more than 10 years. He had undergone a radiofrequency catheter ablation procedure 10 years ago for these frequent VPCs without success at another hospital. He had received intensive heart failure medications including beta-blockers, angiotensin-converting enzyme inhibitors and spironolactone from a local hospital during the last two years.
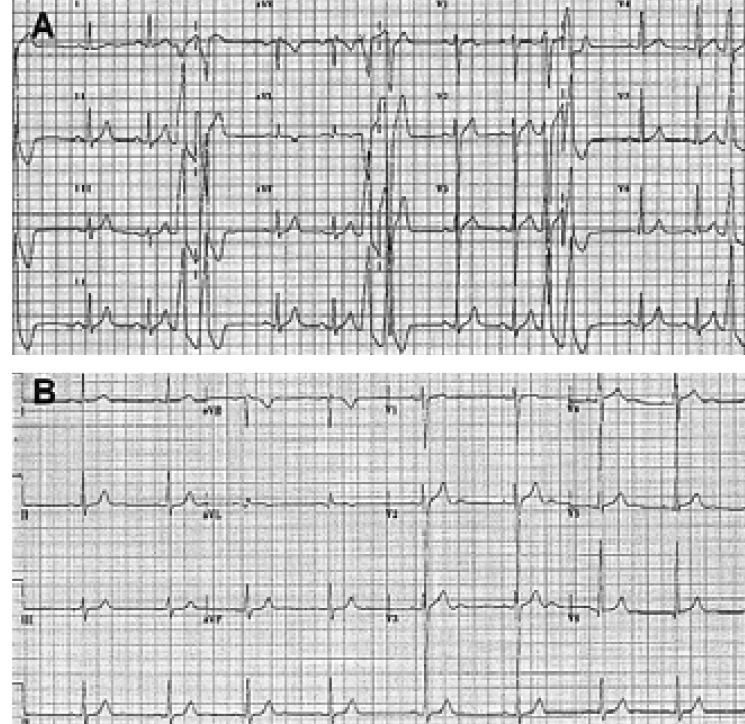
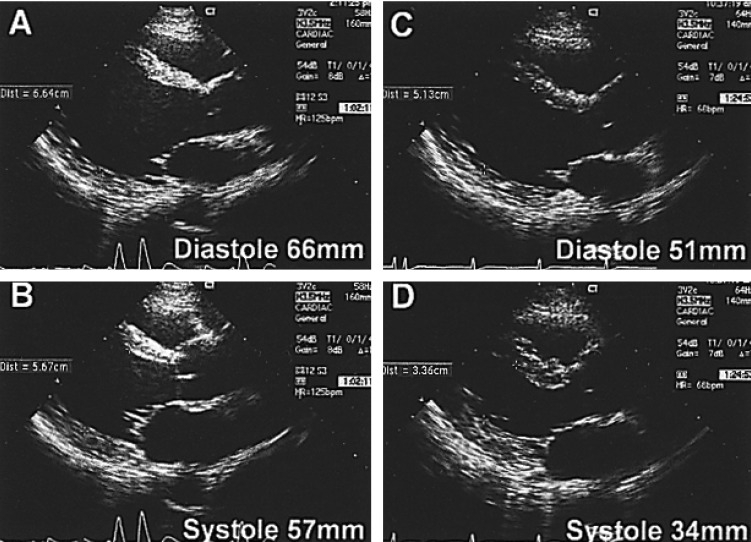
A physical examination revealed jugular vein engorgement and slightly rapid and irregular heart sounds. His vital signs were as follows: a blood pressure of 110/70 mmHg, a pulse rate of 88 beats/min and a respiration rate of 21 breaths/min. The standard 12-lead electrocardiography (ECG) revealed frequent VPCs. The right ventricular outflow tract was suspected as being the origin of this condition due to the negative deflection of the VPCs in lead V1, the positive deflection in leads II, III and aVF, and the QRS transition in lead V4 (Figure 1A). The chest X-ray revealed cardiomegaly and increased broncho-vascular markings. The echocardiography demonstrated dilatation of the left ventricle (LV) and a decreased LV contractile function (LV end-diastolic dimension: 66 mm, LV end-diastolic volume: 211 mL and an ejection fraction: 34%) (Figure 2A). A 24 hour ambulatory ECG showed very frequent VPCs; there were 22,256 isolated VPCs and 16,081 couplets out of 123,139 total heart beats (31%) during 22 hours.
Electrophysiological Study and Radiofrequency Catheter Ablation
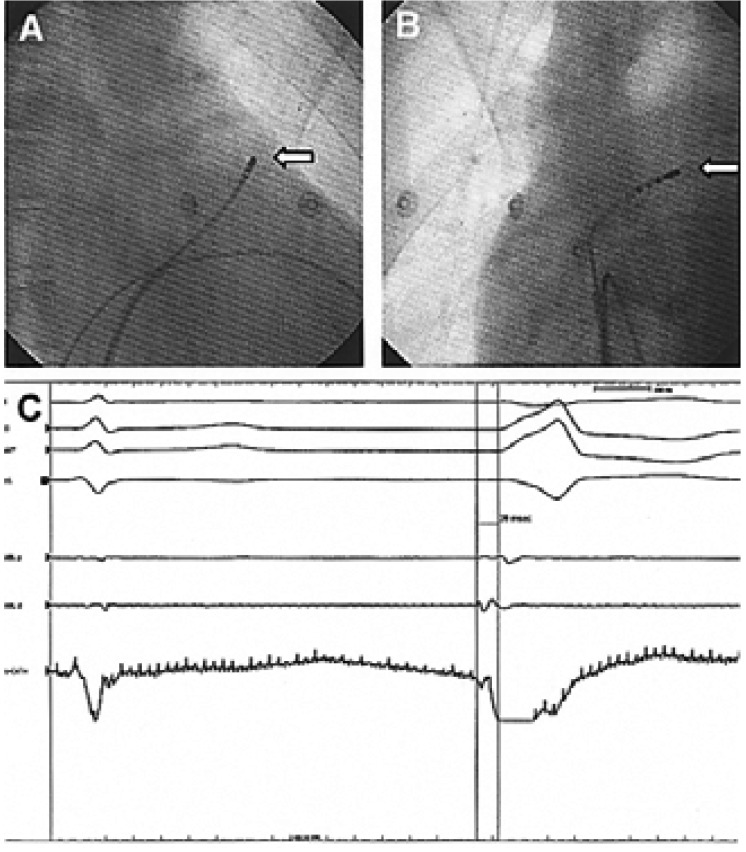
An electrophysiological study and radiofrequency catheter ablation were performed after obtaining an informed written consent on the following day after hospital admission. A 6 Fr. Quadripolar electrode catheter was positioned in the right ventricular (RV) apex. A 7 Fr. deflectable quadripolar ablation catheter (Boston Scientific EP Technologies, Natick, Massachusetts) with a 4-mm-tip electrode was introduced percutaneously into the RV using an 8 Fr. SR0 sheath (Daig®). The origin of the spontaneous VPCs was determined based on the 12-lead-surface ECG and it was further located with the mapping catheter that was placed into the RV outflow tract. The triggering focus of the VPCs was located in the high anteroseptal region (Figure 3A, 3B).
The electrograms recorded from the ablation catheter were very tiny in the area that was mapped, and this was probably due to the scar formation created by the previous unsuccessful radiofrequency catheter ablation. The onset of the bipolar electrogram of the spontaneous VPCs recorded by the ablation catheter was 38 ms earlier than that of the surface ECG, and the unipolar electrogram had abrupt negative deflections without an initial positive component at the site we chose for ablation (Figure 3C). Radiofrequency energy was delivered for 60 seconds with a preset temperature of 60℃ and power limit of 40 W. The VPCs disappeared within 5 seconds after reaching a tissue-electrode temperature of 50℃. A booster application of energy was delivered to four sites around the successfully ablated focus for 30 seconds each.
Immediate progress and Follow-up
A 24 hour ambulatory ECG taken the same day as the radiofrequency catheter ablation procedure recorded only a few atrial premature complexes without any VPCs. The medications that has been administered for heart failure before the treatment were continued thereafter. No VPCs were observed throughout a series of ECGs that were recorded during the 6 months following his discharge. The LV dimensions and function returned to normal, as determined by the 6 month follow-up echocardiography: the LV end-diastolic dimension was 51 mm and the ejection fraction was 55% (Figure 2B).
DISCUSSION
Chronic supraventricular and ventricular tachycardias can lead to congestive cardiomyopathy in animal models4) and in humans too5). Sustained rapid atrial or ventricular pacing in animals results in systolic heart failure that is neurohormonally and hemodynamically similar to the left ventricular systolic failure seen in humans6-8). The characteristic cardiac morphologic alterations in dogs include dilation of all 4 chambers and a normal or reduced ventricular wall thickness, with little or no change in the myocardial mass8, 9). The cellular changes include the loss of myocytes, cellular elongation, myofibril misalignment and the loss of the sarcomere register7), which may be due to the derangement of the extracellular matrix. One of the proposed mechanisms for tachycardia-induced cardiomyopathy involves myocardial energy depletion and impaired energy utilization; this is manifested as reduced myocardial energy stores (including creatine, phosphocreatine and adenosine triphosphate), enhanced activity of the Krebs cycle oxidative enzymes, mitochondrial structural injury and functional abnormalities7, 10). The contractile reserve in response to inotropic agents, volume loading and postextrasystolic potentiation is either diminished or absent11). Reductions in the beta-adrenergic receptor density and also postreceptor abnormalities of adenylate cyclase and calcium processing that decrease the cardiac sympathetic responsiveness have been observed as well12, 13). It is not clear, however, if these factors lead to cardiac dysfunction or if they are merely a consequence of rapid pacing. Myocardial ischemia may impair the systolic function in the presence of a supraphysiologic heart rate, reduced systemic arterial pressure or increased ventricular diastolic pressure14, 15). Abnormal calcium processing may be responsible for tachycardia-induced cardiomyopathy. Extensive abnormalities of calcium channel activity and calcium transport in the sarcoplasmic reticulum appear as early as 24 hours after the initiation of rapid pacing, and these abnormalities may persist for up to 4 weeks after the discontinuation of pacing10, 16). The severity of the calcium cycling abnormalities correlates with the degree of ventricular dysfunction10). In this manner, the calcium available to the myocytes may be decreased, with a subsequent reduction in the contractility. In the clinical field, achieving pharmacological control17) and elimination of these tachycardias via surgical18) or transcatheter ablation19, 20) have demonstrated that this tachycardia-induced phenomenon is surely reversible.
Although the presence of VPCs has been found to be an independent risk factor for sudden death occurring for the patient who is in a post-myocardial infarction status, isolated VPCs are known to be the most common and benign arrhythmia that doctors encounter in routine examinations21, 22). Further, there is only minimal risk of VPCs, and especially right ventricular extrasystoles, in the patients without structural heart disease23). A series of patients with RVOT-VPC have recently been reported on. This was a common arrhythmia in that report, and it was able to cause LV dilation1), which is a well-recognized precursor of LV dysfunction and heart failure. We experienced and report here on a patient with VPC-induced cardiomyopathy, whose left ventricle was not only dilated, but it was also accompanied with severe functional impairment. Although the frequency of the VPCs in our patient was similar to that in the previous report, our patient had suffered from them for a much longer duration than in the previous report (> 10 years vs. < 2 years, respectively). The LV dimension and function in our case completely recovered within six months after eliminating the RVOT-VPCs with performing radiofrequency catheter ablation. VPCs are one of the most common and benign arrhythmias, and they can cause marked LV dilation and severe functional impairment even in structurally normal hearts when they are very frequent and longstanding phenomena. RFCA should be the therapy of choice to treat this malady in this type of patient.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





